Muscle Energy Technique (MET)
Introduction
Muscle Energy Technique (MET) is a widely used manual therapy intervention in physiotherapy and musculoskeletal rehabilitation that employs voluntary, controlled muscle contractions by the patient against a precisely directed counterforce provided by the therapist. Unlike passive manual techniques, MET is an active approach that integrates patient participation, neuromuscular control, and biomechanical specificity to address joint dysfunction, muscle tightness, altered length–tension relationships, and restricted mobility.
MET is particularly valued for its safety profile, precision, and adaptability across acute, subacute, and chronic conditions. It is commonly incorporated into orthopedic, spinal, sports, and neurological rehabilitation programs, either as a standalone technique or in combination with mobilization, stretching, and strengthening interventions.
Definition
Muscle Energy Technique is defined as a manual therapy method in which the patient actively contracts specific muscles, in a controlled manner and direction, against a therapist-applied resistance, to achieve therapeutic effects such as improved mobility, reduced muscle tone, and correction of joint dysfunction.
Key defining elements include:
- Active patient participation
- Submaximal, controlled isometric or isotonic contractions
- Precise therapist positioning and stabilization
- Specific therapeutic intent (lengthening, mobilization, or alignment correction)
Therapeutic Objectives and Clinical Rationale
The primary objectives of MET include:
- Reducing muscle tightness and hypertonicity
- Improving joint range of motion
- Normalizing muscle length–tension relationships
- Addressing joint hypomobility and positional dysfunctions
- Enhancing neuromuscular control and coordination
- Reducing pain and movement restriction
- Facilitating postural and biomechanical correction
Clinically, MET is particularly effective when restricted mobility is associated with muscle guarding, adaptive shortening, or neuromuscular imbalance, rather than purely structural limitation.
Mechanism of Action
The therapeutic effects of MET are explained through several interrelated mechanisms:
Post-Isometric Relaxation
Following an isometric muscle contraction, there is a temporary reduction in muscle tone, allowing the muscle to be lengthened more effectively.
Reciprocal Inhibition
Contraction of the agonist muscle inhibits the antagonist via spinal reflex pathways, facilitating improved extensibility of the opposing muscle group.
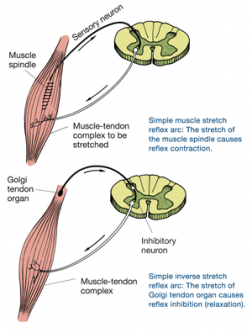
Golgi Tendon Organ Activation
Isometric contraction stimulates Golgi tendon organs, contributing to autogenic inhibition and reduced muscle tension.
Joint Mechanoreceptor Stimulation
Active contraction and therapist-controlled movement enhance afferent input from joint receptors, improving sensorimotor integration.
Motor Control Re-education
Patient participation reinforces correct movement patterns and neuromuscular coordination.
Indications and Clinical Applications
MET is indicated in a wide range of conditions:
Spinal Conditions
- Cervical, thoracic, and lumbar segmental dysfunction
- Mechanical neck and back pain
- Postural asymmetries
- Sacroiliac joint dysfunction
Peripheral Joint Conditions
- Shoulder capsular tightness
- Hip flexor and hamstring tightness
- Knee and ankle mobility restrictions
- Post-immobilization stiffness
Muscle and Soft Tissue Disorders
- Adaptive muscle shortening
- Myofascial tightness
- Muscle imbalance syndromes
Sports Rehabilitation
- Limited range following strain injuries
- Movement asymmetries affecting performance
Contraindications and Precautions
Absolute Contraindications
- Acute fractures
- Severe joint instability
- Acute inflammatory or infective conditions
- Recent surgical repair where contraction is contraindicated
Relative Contraindications / Precautions
- Acute muscle strain (early phase)
- Severe pain with contraction
- Osteoporosis (especially spinal MET)
- Neurological conditions with poor motor control
Force levels should always be submaximal and symptom-guided.
Assessment Prerequisites
Before applying MET, the therapist should assess:
- Joint range of motion and end-feel
- Muscle length and tone
- Pain behavior and irritability
- Movement asymmetry and alignment
- Patient’s ability to understand and perform controlled contractions
Accurate assessment ensures correct muscle selection and technique specificity.
Principles of Application
Effective MET application is guided by the following principles:
- Precise positioning and stabilization
- Use of gentle, submaximal contractions (typically 20–30% effort)
- Pain-free execution of contractions
- Clear verbal instruction and patient feedback
- Gradual progression of range after relaxation
- Reassessment after each repetition
MET should feel controlled and comfortable, not forceful.
Types of Muscle Energy Technique


4
Post-Isometric Relaxation (PIR)
The patient performs an isometric contraction of the restricted muscle, followed by relaxation and passive movement into the new range.
Reciprocal Inhibition MET
The patient contracts the antagonist muscle to facilitate relaxation and lengthening of the tight agonist.
Isotonic MET
Controlled concentric or eccentric contractions are used to improve strength and range in specific patterns.
Joint-Specific MET
Applied to address positional faults or hypomobility at specific joints or spinal segments.
Dosage Parameters
Typical MET dosage guidelines include:
- Contraction duration: 5–10 seconds
- Intensity: 20–30% of maximal effort
- Repetitions: 3–5 per muscle or joint
- Sets: 1–2
- Rest: Short relaxation phase between repetitions
Progression involves improved range, better control, and integration into functional movement.
Integration into Rehabilitation Programs
MET is most effective when integrated with:
- Stretching and flexibility exercises
- Joint mobilization techniques
- Strengthening and conditioning programs
- Postural correction strategies
- Functional movement retraining
MET often serves as a preparatory technique to improve movement quality before active exercise.
Outcome Measures and Monitoring
Effectiveness can be monitored using:
- Goniometric range of motion
- Palpation of muscle tone
- Functional movement assessment
- Patient-reported pain and ease of movement
Immediate reassessment after MET is essential to confirm benefit.
Advantages and Limitations
Advantages
- Safe and gentle technique
- High patient involvement
- Precise and joint-specific
- Effective for muscle-related restrictions
Limitations
- Limited effect on fixed structural restrictions
- Requires patient cooperation and understanding
- Technique-dependent therapist skill
- Effects may be short-term without follow-up exercise
Clinical Pearls
- Less force produces better results in MET
- Precision is more important than strength
- Reassess after each repetition
- Follow MET with active control exercises
- MET is most effective for neuromuscular, not structural, restriction
Conclusion
Muscle Energy Technique is a valuable, evidence-informed manual therapy intervention that leverages active patient participation to address muscle tightness, joint restriction, and movement dysfunction. When applied with accurate assessment, precise execution, and appropriate integration into rehabilitation programs, MET enhances mobility, reduces pain, and supports efficient, controlled movement.
References
- Chaitow L, Crenshaw K. Muscle Energy Techniques. Elsevier.
- Kisner C, Colby L, Borstad J. Therapeutic Exercise: Foundations and Techniques.
- Magee D. Orthopedic Physical Assessment.
- Greenman PE. Principles of Manual Medicine.
- Fryer G. Muscle energy technique: An evidence-informed approach. Int J Osteopath Med.