

MOTOR ASSESSMENT SCALE (MAS)
A Comprehensive Clinical Guide for Physiotherapists
1. Introduction and Clinical Importance
In neurological rehabilitation, clinicians must evaluate not only impairment but also how effectively a patient performs functional motor tasks. While impairment-level tools (e.g., strength or synergy-based assessments) quantify deficits, task-oriented tools capture functional motor performance, which is often more directly linked to independence and participation.
The Motor Assessment Scale (MAS) is a stroke-specific, performance-based assessment designed to evaluate everyday motor tasks commonly addressed in physiotherapy. It emphasizes task completion and movement efficiency, making it particularly valuable for goal setting, treatment planning, and outcome monitoring in stroke rehabilitation.
Within a physiotherapy intranet, the MAS should be presented as a core functional motor assessment tool, complementary to impairment-based measures such as the Fugl–Meyer Assessment.
2. Purpose of the Motor Assessment Scale
The MAS is designed to:
• Assess functional motor performance after stroke
• Evaluate the ability to perform key everyday motor tasks
• Monitor progress over time in response to therapy
• Support task-oriented rehabilitation approaches
• Provide standardized outcome data for clinical practice and research
The MAS focuses on what the patient can do, rather than isolated neuromuscular impairments.
3. Theoretical Basis
The MAS is grounded in principles of motor relearning and task-specific training, emphasizing:
• Active problem-solving
• Practice of functional tasks
• Adaptation and efficiency of movement
Unlike impairment-based scales, the MAS does not prioritize synergy patterns or reflex activity; it reflects functional task mastery.
4. Constructs Measured
The MAS measures:
• Functional motor task performance
• Trunk control
• Upper limb task execution
• Lower limb and gait-related tasks
It does not directly assess:
• Muscle strength in isolation
• Sensory impairment
• Pain or range of motion
These domains require additional tools.
5. Indications and Patient Populations
The MAS is appropriate for:
• Acute, subacute, and chronic stroke
• Inpatient and outpatient neurorehabilitation
• Community-based stroke rehabilitation
• Research and outcome monitoring in stroke
It is less suitable for:
• Non-stroke neurological conditions
• Very severe cognitive impairment
• Patients unable to follow instructions
6. Structure and Scoring Overview
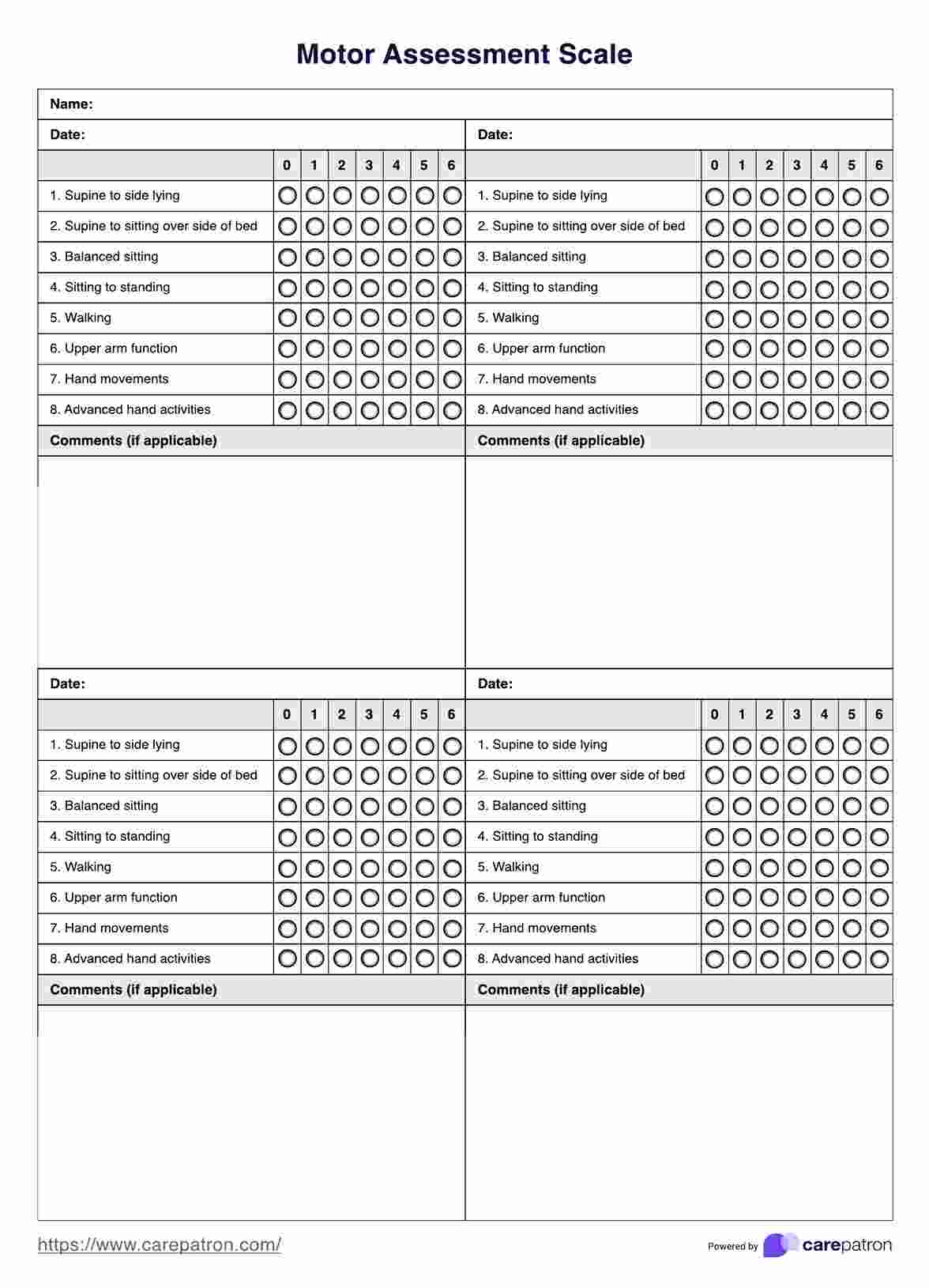
The MAS consists of 8 functional items, each scored on a 7-point ordinal scale (0–6).
MAS Items
- Supine to side-lying
- Supine to sitting over side of bed
- Balanced sitting
- Sitting to standing
- Walking
- Upper arm function
- Hand movements
- Advanced hand activities
Maximum total score: 48 points
Higher scores indicate better functional motor performance.
7. Equipment and Test Setup
Equipment Required
• Bed or plinth
• Chair (with or without armrests)
• Stopwatch
• Small objects (coin, pencil, cup)
• Clear walking area
Environment
• Quiet and well-lit
• Adequate space for transfers and walking
• Safe, non-slip floor
8. Step-by-Step Administration Procedure
Step 1: Patient Preparation
• Explain each task clearly
• Demonstrate if required
• Ensure patient safety at all times
Step 2: Task Administration
• Perform items in the standardized order
• Allow rest breaks between tasks
• Observe movement quality and task completion
Step 3: Scoring Each Item
Each item is scored 0–6, based on predefined performance criteria.
General interpretation:
• 0 – Unable to perform the task
• 6 – Performs task normally and efficiently
Score based on:
• Task completion
• Speed
• Control and coordination
Step 4: Recording the Score
Document:
• Individual item scores
• Total MAS score
• Use of aids or compensations
Example:
“MAS total: 32/48; difficulty noted in advanced hand activities.”
9. Correct Scoring and Common Errors
Correct Practice
• Use standardized scoring criteria
• Score actual performance, not potential ability
• Avoid providing physical assistance during testing
Common Errors
• Over-scoring partially completed tasks
• Coaching excessively during assessment
• Ignoring compensatory strategies
10. Interpretation of MAS Scores
Clinical Interpretation
• Lower scores indicate greater functional limitation
• Item-level scores help identify task-specific deficits
• Changes in individual items may be more clinically meaningful than total score alone
The MAS does not have universal cut-off scores; interpretation should be goal- and task-oriented.
11. Reliability of the MAS
Inter-Rater Reliability
• ICC values: 0.96–0.99
Test–Retest Reliability
• ICC values: 0.95–0.98
These findings demonstrate excellent reliability when standardized instructions are followed.
12. Validity of the MAS
Content Validity
• Strong alignment with functional motor tasks relevant to daily life
Construct Validity
• Moderate to strong correlations with:
– Fugl–Meyer Assessment
– Functional Independence Measure
– Gait and balance measures
Correlation coefficients typically range from 0.65 to 0.85.
13. Responsiveness and Clinically Important Change
Responsiveness
The MAS is responsive to:
• Task-specific training
• Functional strengthening
• Neurorehabilitation interventions
Clinically Meaningful Change
• An improvement of ≥1 point in an item
• Or ≥3–4 points in total score is generally considered clinically meaningful
14. Clinical Decision-Making Using the MAS
MAS results guide:
• Selection of functional tasks for training
• Progression from basic to advanced activities
• Upper limb functional goal setting
• Discharge readiness assessment
Examples:
• Low trunk item scores → emphasize core control and transfers
• Low hand scores → prioritize fine motor and grasp training
• Improving MAS with stable FMA → functional compensation occurring
15. SOAP-Based Documentation Example
S:
Patient reports difficulty using affected hand for daily activities.
O:
MAS: Hand movements 3/6; advanced hand activities 2/6.
A:
Reduced functional hand use limiting ADLs.
P:
Task-oriented upper limb training focusing on grasp and release. Reassess MAS in 2–3 weeks.
16. Reassessment and Outcome Tracking
Recommended reassessment:
• Every 2–4 weeks
• At functional milestones
• Pre-discharge
The MAS complements:
• Fugl–Meyer Assessment (impairment)
• ADL scales (participation)
17. Advantages and Limitations
Advantages
• Strong functional relevance
• Excellent reliability and validity
• Sensitive to change
• Easy to administer compared to impairment scales
Limitations
• Stroke-specific
• Less detailed impairment analysis
• Ceiling effect in high-functioning patients
18. Key Clinical Takeaways
• MAS is a task-oriented functional motor assessment for stroke
• Complements impairment-based measures
• Demonstrates excellent reliability and validity
• Item-level changes are clinically meaningful
• Ideal for guiding functional rehabilitation goals
19. Key Literature References
- Carr JH, Shepherd RB, Nordholm L, Lynne D. Investigation of a new motor assessment scale for stroke patients. Physical Therapy. 1985;65(2):175–180.
- Poole JL, Whitney SL. Motor Assessment Scale for stroke: Reliability and validity. Physical Therapy. 1988;68(9):1352–1357.
- Carr JH, Shepherd RB. Stroke Rehabilitation: Guidelines for Exercise and Training to Optimize Motor Skill. Butterworth-Heinemann; 2003.
- Tyson S, Connell L. The psychometric properties and clinical utility of measures of walking and mobility in neurological conditions. Clinical Rehabilitation. 2009;23(11):1018–1033.
- Langhorne P, Bernhardt J, Kwakkel G. Stroke rehabilitation. The Lancet. 2011;377(9778):1693–1702.