
4
FUNCTIONAL INDEPENDENCE MEASURE (FIM)
A Comprehensive Clinical Guide for Physiotherapists
1. Introduction and Clinical Importance
Rehabilitation outcomes must extend beyond impairment reduction to demonstrate meaningful functional independence. Health systems, insurers, and interdisciplinary teams require standardized measures that quantify burden of care, assistance needs, and functional gains across time.
The Functional Independence Measure (FIM) is a globally recognized functional outcome measure that evaluates a patient’s level of independence across motor and cognitive domains. It is extensively used in inpatient rehabilitation, neurological recovery, and post-acute care pathways to guide goal setting, discharge planning, and outcome benchmarking.
Within a physiotherapy intranet, the FIM should be positioned as a core multidisciplinary functional outcome tool, with physiotherapists primarily responsible for the motor domain interpretation and application.
2. Purpose of the FIM
The FIM is designed to:
• Quantify functional independence
• Measure burden of care
• Track functional change over time
• Support goal setting and discharge planning
• Enable standardized reporting for audits and reimbursement
The FIM focuses on what the patient actually does, not capacity under ideal conditions.
3. Constructs Measured
The FIM evaluates two major domains:
A. Motor Domain (13 items)
• Self-care
• Sphincter control
• Transfers
• Locomotion
B. Cognitive Domain (5 items)
• Communication
• Social cognition
Physiotherapists primarily contribute to:
• Transfers
• Locomotion
• Elements of self-care (in collaboration with OT)
4. Indications and Patient Populations
The FIM is appropriate for:
• Stroke and neurological rehabilitation
• Traumatic brain injury
• Spinal cord injury
• Orthopaedic and post-surgical rehabilitation
• Geriatric inpatient rehabilitation
• Post-ICU functional assessment
It is less suitable for:
• Very high-functioning individuals (ceiling effect)
• Rapid screening contexts
5. Structure and Scoring Overview
The FIM consists of 18 items, each scored on a 7-point ordinal scale.
Scoring Levels
• 7 – Complete Independence
• 6 – Modified Independence (device/time)
• 5 – Supervision or setup
• 4 – Minimal assistance (≥75% effort)
• 3 – Moderate assistance (50–74%)
• 2 – Maximal assistance (25–49%)
• 1 – Total assistance (<25%)
Total Score Range
• Minimum: 18
• Maximum: 126
Higher scores indicate greater independence and lower care burden.
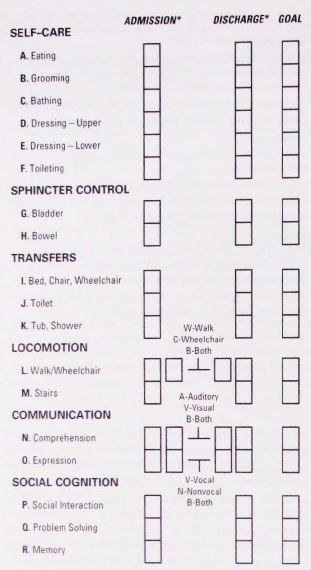
6. FIM Items (Overview)
Motor Items (13)
- Eating
- Grooming
- Bathing
- Dressing – upper body
- Dressing – lower body
- Toileting
- Bladder management
- Bowel management
- Transfers – bed/chair/wheelchair
- Transfers – toilet
- Transfers – tub/shower
- Locomotion – walk/wheelchair
- Stairs
Cognitive Items (5)
- Comprehension
- Expression
- Social interaction
- Problem solving
- Memory
7. Equipment and Information Sources
Information Sources
• Direct observation (preferred)
• Nursing and caregiver input
• Therapy session performance
Equipment
• Standard ward and therapy equipment
• Assistive devices used by the patient
No special tools are required.
8. Step-by-Step Administration Procedure
Step 1: Define Observation Period
Score based on usual performance over the last 24 hours, not best or worst effort.
Step 2: Observe or Confirm Performance
Use:
• Direct task observation
• Corroborated reports from staff/caregivers
Avoid scoring based solely on therapy-session performance if it differs from ward function.
Step 3: Assign Item Scores
Score each item based on:
• Level of assistance required
• Use of devices
• Time taken and safety
Supervision or setup automatically limits the score to 5 or below.
Step 4: Calculate Domain and Total Scores
• Sum motor domain scores
• Sum cognitive domain scores
• Calculate total FIM score
Document both total and domain-specific scores.
9. Correct Scoring and Common Errors
Correct Practice
• Score actual performance, not potential ability
• Distinguish supervision from physical assistance
• Apply the lowest appropriate score when variability exists
Common Errors
• Over-scoring independence
• Ignoring setup or safety supervision
• Confusing modified independence (6) with complete independence (7)
10. Interpretation of FIM Scores
Functional Interpretation (General)
• 18–60: Severe dependence
• 61–90: Moderate dependence
• 91–120: Mild dependence
• 121–126: Near-complete independence
Interpretation should focus on care burden, not just numerical change.
11. Reliability of the FIM
Inter-Rater Reliability
• ICC values: 0.85–0.97 across items
• Higher reliability when assessors are trained
Test–Retest Reliability
• ICC values: 0.90–0.98
Clinical implication:
The FIM provides reliable functional tracking when standardized scoring criteria are applied.
12. Validity of the FIM
Content Validity
• Broad coverage of functional domains relevant to rehabilitation
Construct Validity
• Strong correlations with:
– Barthel Index
– Disability Rating Scale
– Length of stay and discharge destination
Correlation coefficients commonly range from 0.70 to 0.90.
13. Responsiveness and MCID
Responsiveness
The FIM is responsive to:
• Inpatient rehabilitation programs
• Task-specific functional training
• Multidisciplinary intervention
Minimal Clinically Important Difference (MCID)
• Reported MCID: ≈22 points (total FIM) in inpatient rehabilitation
• Smaller changes may still be meaningful at item or domain level
14. Clinical Decision-Making Using the FIM
FIM scores guide:
• Therapy intensity and prioritization
• Discharge planning and destination
• Caregiver training needs
• Equipment and environmental modifications
Examples:
• Low transfer FIM → focus on bed mobility and sit-to-stand
• Improving motor FIM with stable cognitive FIM → physical recovery dominant
• Plateauing FIM → reassess barriers (environmental, cognitive, medical)
15. SOAP-Based Documentation Example
S:
Patient reports difficulty performing transfers independently.
O:
FIM transfer (bed/chair): 3/7; locomotion: 4/7.
A:
Moderate assistance required for transfers and ambulation.
P:
Progressive transfer training and gait practice. Reassess FIM in 2 weeks.
16. Reassessment and Outcome Tracking
Recommended reassessment:
• On admission
• Every 2–3 weeks in inpatient rehab
• At discharge
FIM change scores are valuable for:
• Program evaluation
• Benchmarking outcomes
• Quality assurance
17. Advantages and Limitations
Advantages
• Comprehensive functional assessment
• Strong reliability and validity
• Widely accepted internationally
• Useful for discharge and care planning
Limitations
• Licensing and training requirements in some regions
• Ceiling effect in high-functioning patients
• Less sensitive to small functional changes
18. Key Clinical Takeaways
• FIM is a cornerstone functional outcome measure in rehabilitation
• Quantifies independence and burden of care
• Demonstrates strong psychometric properties
• MCID ≈ 22 points in inpatient settings
• Essential for discharge planning and outcome reporting
19. Key Literature References
- Keith RA, Granger CV, Hamilton BB, Sherwin FS. The Functional Independence Measure: A new tool for rehabilitation. Advances in Clinical Rehabilitation. 1987;1:6–18.
- Dodds TA, Martin DP, Stolov WC, Deyo RA. A validation of the Functional Independence Measurement and its performance among rehabilitation inpatients. Archives of Physical Medicine and Rehabilitation. 1993;74(5):531–536.
- Granger CV, Hamilton BB, Keith RA, Zielezny M, Sherwin FS. Advances in functional assessment for medical rehabilitation. Topics in Geriatric Rehabilitation. 1986;1(3):59–74.
- Ottenbacher KJ, Hsu Y, Granger CV, Fiedler RC. The reliability of the Functional Independence Measure: A quantitative review. Archives of Physical Medicine and Rehabilitation. 1996;77(12):1226–1232.
- Stineman MG, Shea JA, Jette A, et al. The Functional Independence Measure: Tests of scaling assumptions, structure, and reliability across 20 diverse impairment categories. Archives of Physical Medicine and Rehabilitation. 1996;77(11):1101–1108.