
BERG BALANCE SCALE (BBS)
A Comprehensive Clinical Guide for Physiotherapists
1. Introduction and Clinical Importance
Balance impairment is a major contributor to falls, activity limitation, fear of movement, and loss of independence across neurological, geriatric, and orthopaedic populations. Accurate and standardized assessment of balance is therefore essential for clinical reasoning, intervention planning, and outcome evaluation.
The Berg Balance Scale (BBS) is one of the most widely used performance-based balance assessment tools in physiotherapy. It evaluates both static and dynamic balance tasks that are representative of everyday functional activities. Due to its strong psychometric properties and clinical feasibility, the BBS is considered a core balance assessment tool for rehabilitation settings worldwide.
2. Purpose of the Berg Balance Scale
The BBS is designed to:
• Assess static and dynamic balance abilities
• Identify fall risk
• Monitor changes in balance over time
• Guide progression of balance and mobility training
• Support objective documentation and discharge decisions
The scale emphasizes functional balance performance, not isolated postural reflexes or sensory systems.
3. Constructs Measured
The BBS measures the following balance-related constructs:
• Static balance (sitting and standing)
• Dynamic balance during functional tasks
• Postural control during transfers
• Weight shifting and reaching
• Transitional movements
It does not directly assess:
• Gait adaptability
• Reactive balance responses
• Dual-task balance performance
These domains may require supplementary tools.
4. Indications and Patient Populations
The BBS is appropriate for use in:
• Stroke and other neurological conditions
• Parkinson’s disease
• Geriatric rehabilitation
• Vestibular disorders
• Orthopaedic and post-surgical rehabilitation
• Community-dwelling older adults
Patient Prerequisites
The patient should be able to:
• Sit unsupported
• Stand with or without minimal assistance
• Follow simple verbal instructions
The BBS may not be suitable for:
• Non-ambulatory patients
• Very high-functioning individuals (ceiling effect)
• Patients with severe cognitive impairment
5. Description of the Tool
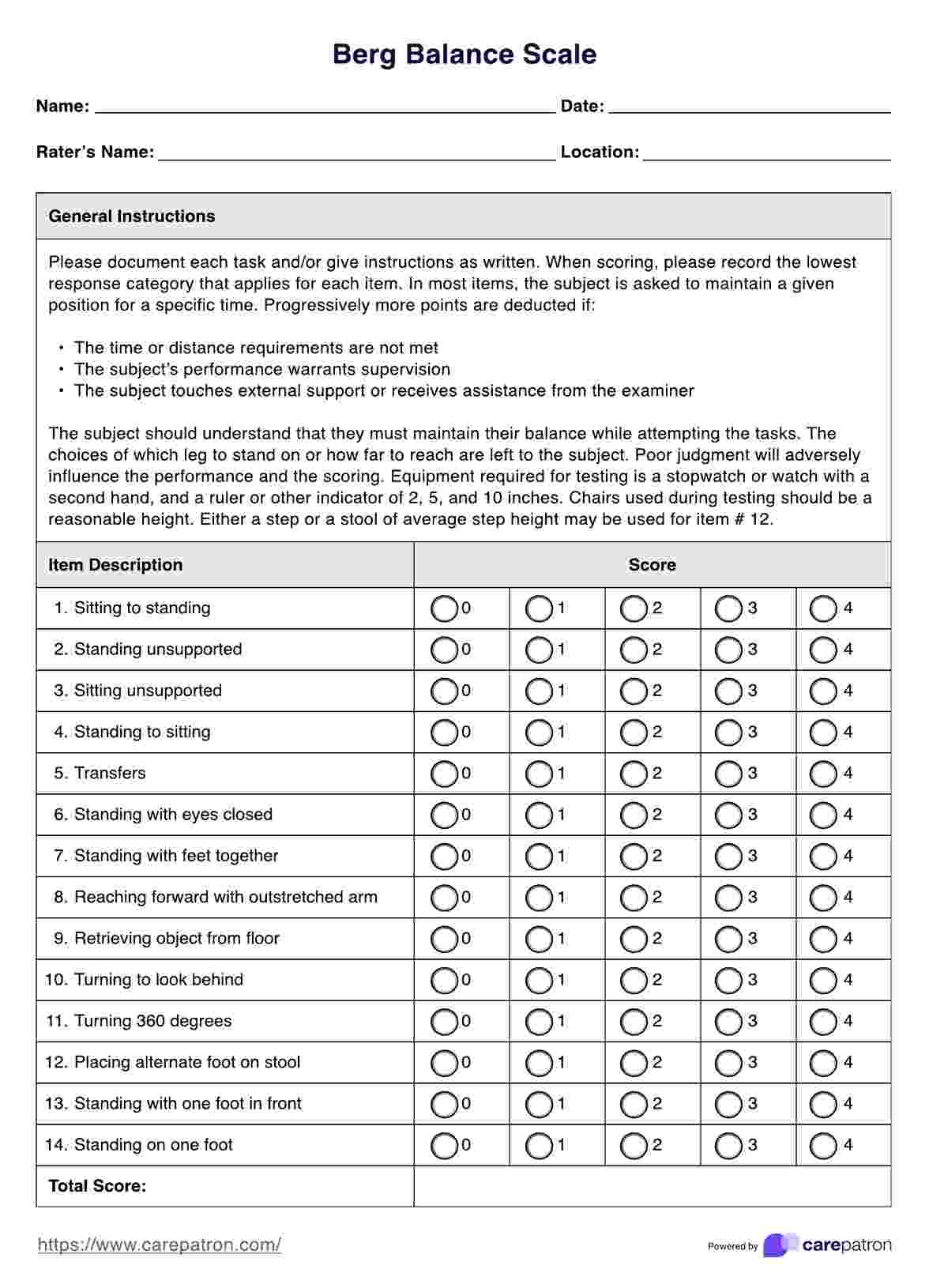
The Berg Balance Scale consists of 14 functional tasks, each scored on a 5-point ordinal scale (0–4).
Total score range: 0–56
Higher scores indicate better balance performance.
6. List of BBS Items
The 14 items include:
- Sitting to standing
- Standing unsupported
- Sitting unsupported
- Standing to sitting
- Transfers
- Standing with eyes closed
- Standing with feet together
- Reaching forward with outstretched arm
- Picking up object from floor
- Turning to look behind
- Turning 360 degrees
- Placing alternate foot on stool
- Standing with one foot in front
- Standing on one leg
These tasks progressively challenge postural stability and dynamic control.
7. Equipment and Test Setup
Required Equipment
• Standard chair with armrests
• Stopwatch
• Ruler or measuring tape
• Step or stool (~20–25 cm height)
• Object to pick up from floor
Environment
• Quiet, well-lit area
• Non-slip flooring
• Adequate space for turning and stepping
Standardization of environment is essential for reliable reassessment.
8. Step-by-Step Administration Procedure
Step 1: Patient Preparation
• Explain the purpose of the test
• Demonstrate each task if required
• Ensure patient safety throughout
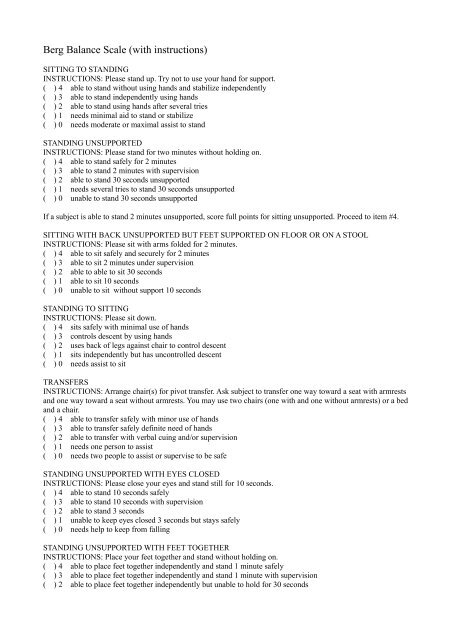
Step 2: Standardized Instructions
• Follow the exact instructions provided in the BBS manual
• Allow one practice attempt if needed
• Provide verbal cues only as specified
Step 3: Task Performance
• Observe quality, control, and safety
• Do not physically assist unless patient safety is compromised
• If assistance is required, score the item accordingly
Step 4: Scoring Each Item
Each item is scored from 0 to 4:
• 0 – Unable to perform
• 1 – Performs with maximal assistance
• 2 – Performs with minimal assistance
• 3 – Performs independently with supervision or time
• 4 – Performs independently and safely
Step 5: Total Score Calculation
Add all item scores to obtain a total out of 56.
Document:
• Total score
• Any observed balance strategies
• Use of assistive devices
9. Correct Scoring and Common Errors
Correct Practice
• Score based on actual performance, not potential ability
• Follow item descriptions strictly
• Maintain consistency across assessments
Common Errors
• Providing physical assistance and scoring as independent
• Deviating from standard instructions
• Rushing item execution
• Ignoring safety observations
10. Interpretation of BBS Scores
General Interpretation
• 41–56: Low fall risk
• 21–40: Medium fall risk
• 0–20: High fall risk
Stroke-Specific Interpretation
• Scores <45 are associated with increased fall risk
• Scores <36 indicate significant balance impairment
Scores should always be interpreted in conjunction with functional mobility and gait assessments.
11. Reliability of the BBS
Inter-Rater Reliability
• ICC: 0.95–0.99
• Demonstrates excellent agreement between examiners
Test–Retest Reliability
• ICC: 0.97–0.98
• High stability across repeated assessments
Clinical implication:
Observed changes in BBS score are highly likely to reflect true balance change, not measurement error.
12. Validity of the BBS
Construct Validity
• Strong correlation with:
– Timed Up and Go Test
– Functional reach
– Gait speed
Correlation coefficients commonly range from 0.67 to 0.91.
Predictive Validity
• BBS scores <45 are predictive of fall risk in older adults and stroke survivors.
13. Responsiveness and MCID
Responsiveness
The BBS is responsive to:
• Balance training
• Strengthening interventions
• Task-specific functional training
Minimal Clinically Important Difference (MCID)
• Stroke population: ≈6–7 points
• Older adults: ≈4–5 points
Changes exceeding these values are considered clinically meaningful.
14. Clinical Decision-Making Using the BBS
BBS results guide:
• Balance training intensity and progression
• Need for supervision or assistive devices
• Fall prevention strategies
• Discharge readiness
Examples:
• BBS <40 → emphasize static and dynamic balance retraining
• Improving BBS with stable TUG → progress gait challenges
• Plateau in BBS → reassess sensory, strength, or cognitive contributors
15. SOAP-Based Documentation Example
S:
Patient reports unsteadiness during standing and turning.
O:
BBS: 38/56; difficulty with single-leg stance and turning.
A:
Moderate balance impairment with increased fall risk.
P:
Initiate progressive balance training and transfer practice. Reassess BBS in 2 weeks.
16. Reassessment and Outcome Tracking
Recommended frequency:
• Every 2–3 weeks in active rehabilitation
• At discharge
• During fall-risk reviews
The BBS should be complemented with:
• Mobility tests (TUG)
• Strength assessments
• ADL measures
17. Advantages and Limitations
Advantages
• Well-validated and widely accepted
• Functional task-based assessment
• Excellent reliability and validity
• Minimal equipment required
Limitations
• Ceiling effect in high-functioning individuals
• Limited assessment of reactive balance
• Time required (~15–20 minutes)
18. Key Clinical Takeaways
• The BBS is a gold-standard functional balance assessment tool
• Demonstrates excellent reliability and validity
• Predictive of fall risk
• MCID ranges from 4–7 points depending on population
• Best used alongside mobility and gait measures
19. Key Literature References
- Berg K, Wood-Dauphinee S, Williams JI, Gayton D. Measuring balance in the elderly: Preliminary development of an instrument. Physiotherapy Canada. 1989;41(6):304–311.
- Berg K, Wood-Dauphinee S, Williams JI. The Balance Scale: Reliability assessment with elderly residents and patients with an acute stroke. Scandinavian Journal of Rehabilitation Medicine. 1995;27(1):27–36.
- Shumway-Cook A, Woollacott M. Motor control: Translating research into clinical practice. 4th ed. Lippincott Williams & Wilkins; 2012.
- Stevenson TJ. Detecting change in patients with stroke using the Berg Balance Scale. Australian Journal of Physiotherapy. 2001;47(1):29–38.
- Donoghue D, Stokes EK. How much change is true change? The minimum detectable change of the Berg Balance Scale in elderly people. Journal of Rehabilitation Medicine. 2009;41(5):343–346.