BARTHEL INDEX
A Comprehensive Clinical Guide for Physiotherapists
1. Introduction and Clinical Importance
Assessment of activities of daily living (ADL) is central to rehabilitation planning, discharge decisions, caregiver training, and outcome reporting. While impairment-level measures describe body function, ADL scales capture how those impairments translate into real-world independence.
The Barthel Index (BI) is one of the most widely used and internationally accepted instruments for measuring functional independence in basic ADLs. Its simplicity, clinical relevance, and strong psychometric properties make it a core outcome measure in neurological, geriatric, orthopedic, and inpatient rehabilitation settings.
Within a physiotherapy intranet, the Barthel Index should be positioned as a mandatory functional outcome tool for baseline assessment, progress monitoring, and discharge documentation.
2. Purpose of the Barthel Index
The Barthel Index is designed to:
• Measure independence in basic activities of daily living
• Quantify burden of care and assistance required
• Monitor functional recovery over time
• Support discharge planning and level-of-care decisions
• Provide standardized data for audits and research
The Barthel Index reflects what the patient actually does, not what they are capable of doing under ideal conditions.
3. Constructs Measured
The Barthel Index measures:
• Self-care independence
• Mobility and transfers
• Continence-related function
It focuses on basic ADLs, not instrumental ADLs (e.g., shopping, cooking).
4. Indications and Patient Populations
The Barthel Index is appropriate for:
• Stroke and neurological rehabilitation
• Geriatric rehabilitation
• Orthopaedic and post-surgical patients
• ICU step-down and inpatient rehabilitation
• Community-based rehabilitation
It is less sensitive in:
• Very high-functioning individuals
• Mild disability states
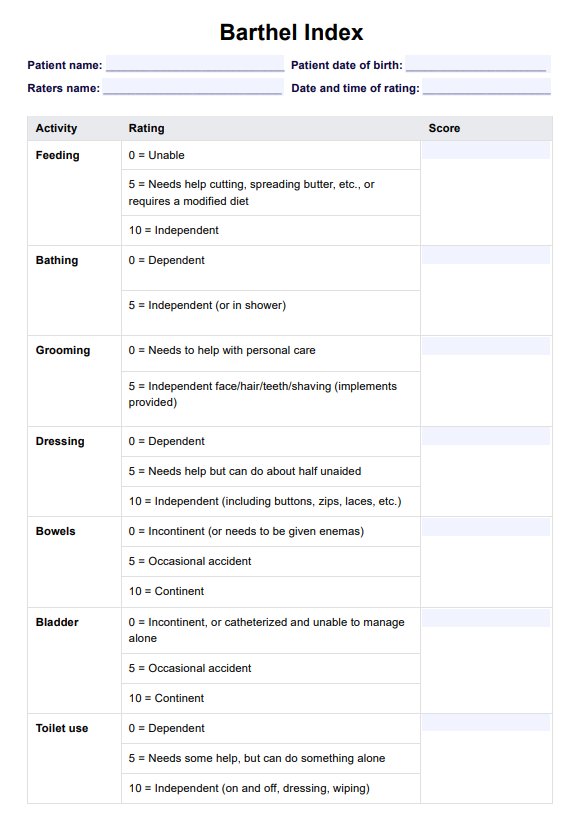
5. Description of the Tool
The Barthel Index consists of 10 ADL items, each scored according to the level of assistance required.
Standard Items Assessed
- Feeding
- Bathing
- Grooming
- Dressing
- Bowels
- Bladder
- Toilet use
- Transfers (bed to chair)
- Mobility (walking or wheelchair)
- Stairs
Scoring Range
• Total score range: 0–100 (or 0–20 in some versions)
• Higher scores indicate greater independence
Consistency in the version used is critical for reassessment.
6. Equipment and Information Sources
The Barthel Index can be completed using:
• Direct observation
• Patient interview
• Caregiver report
• Multidisciplinary input
No specialized equipment is required.
7. Step-by-Step Administration Procedure
Step 1: Define the Time Frame
Assess the patient’s current functional status, not best performance in the past.
Step 2: Gather Information
Use:
• Direct observation during therapy
• Patient self-report
• Caregiver or nursing staff input
Observation is preferred whenever feasible.
Step 3: Score Each Item
Score based on:
• Actual performance
• Level of assistance required
• Use of aids or devices
Do not score based on potential ability.
Step 4: Calculate Total Score
Add scores from all 10 items to obtain the total Barthel Index score.
Document:
• Total score
• Items requiring assistance
• Use of aids or caregiver support
8. Scoring System Explained
Each item is scored in steps (commonly 0, 5, 10, or 15), depending on the task.
Example: Transfers
• 0 – Unable
• 5 – Major help (one or two people)
• 10 – Minor help (verbal or physical)
• 15 – Independent
Precise interpretation of each level is essential to avoid overestimation of independence.
9. Correct Completion and Common Errors
Correct Practice
• Score what the patient does, not what they could do
• Use consistent scoring criteria
• Clarify ambiguous caregiver reports
Common Errors
• Scoring based on therapist assistance during therapy only
• Ignoring supervision needs
• Overestimating independence with assistive devices
10. Interpretation of Barthel Index Scores
Functional Interpretation (0–100 Scale)
• 0–20: Total dependence
• 21–60: Severe dependence
• 61–90: Moderate dependence
• 91–99: Slight dependence
• 100: Independent
These categories support care planning and discharge decisions.
11. Reliability of the Barthel Index
Inter-Rater Reliability
• ICC: 0.90–0.95
• High agreement among clinicians when standardized scoring is used
Test–Retest Reliability
• ICC: 0.89–0.97
• Demonstrates stability over short reassessment intervals
Clinical implication:
Changes in score reflect true functional change, not assessor variability.
12. Validity of the Barthel Index
Content Validity
• Strong coverage of basic ADL domains relevant to rehabilitation
Construct Validity
• Strong correlation with:
– Functional Independence Measure (FIM)
– Mobility and balance measures
Correlation coefficients typically range from 0.70 to 0.90.
13. Responsiveness and MCID
Responsiveness
The Barthel Index is responsive to:
• Functional training
• Task-oriented rehabilitation
• Neurorehabilitation interventions
Minimal Clinically Important Difference (MCID)
• Reported MCID: ≈10–15 points on the 0–100 scale
Changes below this may not reflect meaningful functional improvement.
14. Clinical Decision-Making Using the Barthel Index
Barthel Index scores guide:
• Discharge destination (home vs facility)
• Caregiver assistance requirements
• Therapy intensity and focus
• Goal setting and prioritization
Examples:
• BI <60 → focus on basic self-care and transfers
• Improving BI with stable impairment scores → functional carryover achieved
• Plateauing BI → reassess environmental or cognitive barriers
15. SOAP-Based Documentation Example
S:
Patient reports difficulty with bathing, dressing, and stair climbing.
O:
Barthel Index: 55/100; assistance required for transfers and toileting.
A:
Severe ADL dependence limiting safe home discharge.
P:
Task-specific ADL training, transfer practice, caregiver education. Reassess BI in 2 weeks.
16. Reassessment and Outcome Tracking
Recommended reassessment:
• Every 2–3 weeks in inpatient rehab
• At major functional milestones
• At discharge
The Barthel Index should be used alongside:
• Mobility tests (TUG)
• Balance scales (BBS)
• Strength assessments
17. Advantages and Limitations
Advantages
• Simple and quick to administer
• Minimal training required
• Strong reliability and validity
• Widely accepted internationally
Limitations
• Ceiling effect in high-functioning patients
• Limited sensitivity to small changes
• Does not assess instrumental ADLs
18. Key Clinical Takeaways
• The Barthel Index is a core ADL outcome measure in rehabilitation
• Demonstrates high reliability and good validity
• MCID ≈ 10–15 points
• Essential for discharge planning and care burden estimation
• Best interpreted alongside mobility and balance measures
19. Key Literature References
- Mahoney FI, Barthel DW. Functional evaluation: The Barthel Index. Maryland State Medical Journal. 1965;14:61–65.
- Wade DT, Collin C. The Barthel ADL Index: A standard measure of physical disability? International Disability Studies. 1988;10(2):64–67.
- Quinn TJ, Langhorne P, Stott DJ. Barthel Index for stroke trials: Development, properties, and application. Stroke. 2011;42(4):1146–1151.
- Hsueh IP, Lee MM, Hsieh CL. Psychometric characteristics of the Barthel activities of daily living index in stroke patients. Journal of the Formosan Medical Association. 2001;100(8):526–532.
- Collin C, Wade DT, Davies S, Horne V. The Barthel ADL Index: A reliability study. International