TIMED UP AND GO TEST (TUG)
A Comprehensive Clinical Guide for Physiotherapists
1. Introduction and Clinical Importance
Mobility is a core determinant of functional independence, safety, and quality of life. Impairments in transitional movements, gait initiation, turning, and sit-to-stand performance are strongly associated with falls, functional decline, prolonged hospitalization, and loss of independence—particularly in neurological, geriatric, and post-surgical populations.
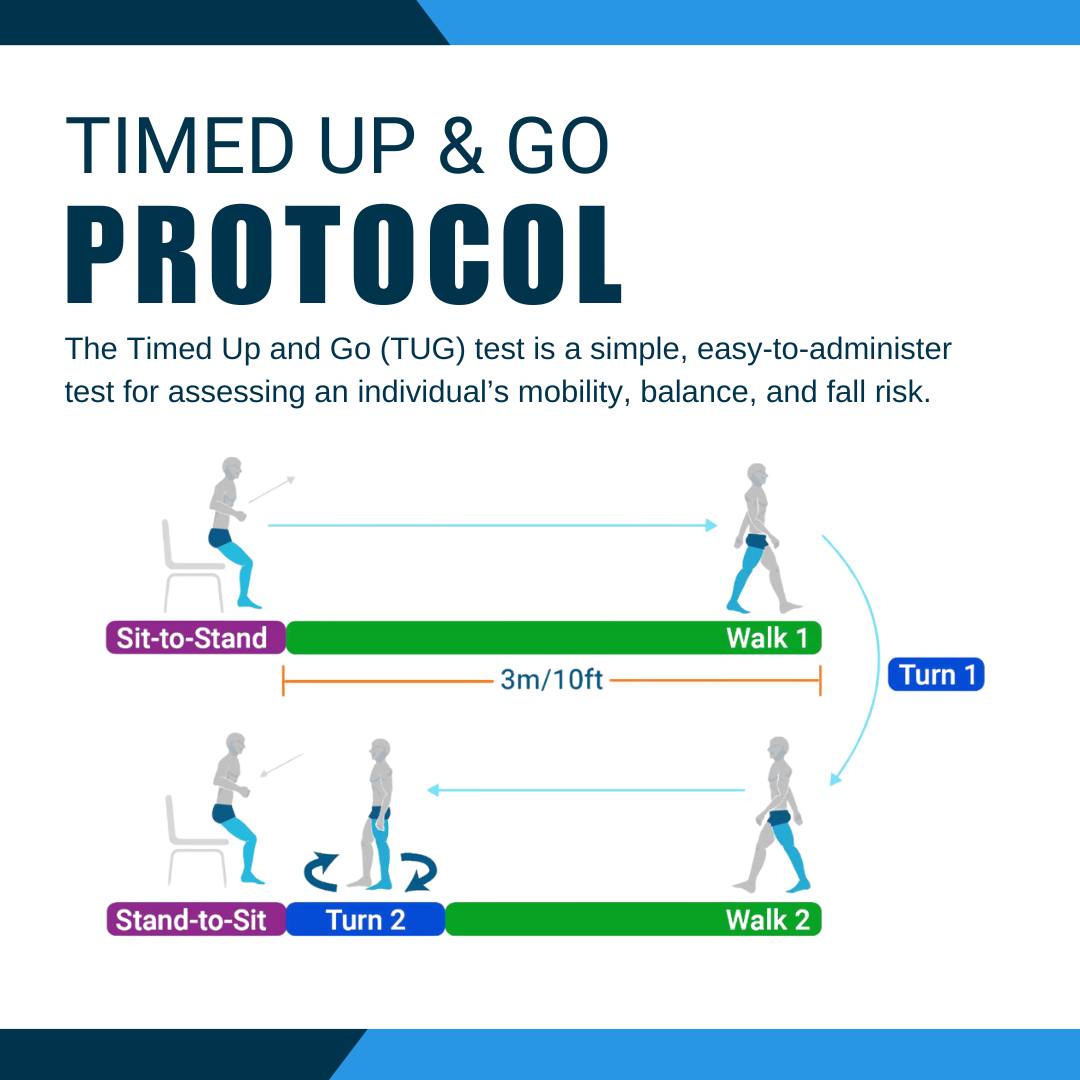
The Timed Up and Go Test (TUG) is a simple, quick, and highly validated functional mobility assessment tool used extensively in physiotherapy practice. It integrates multiple components of functional mobility—sit-to-stand, walking, turning, and stand-to-sit—into a single timed task, making it a powerful screening and outcome measure.
Within an intranet-based physiotherapy knowledge system, the TUG should be considered a mandatory core tool for baseline assessment, reassessment, discharge planning, and fall-risk screening.
2. Purpose of the TUG
The Timed Up and Go Test is designed to:
• Assess functional mobility
• Screen for fall risk
• Evaluate dynamic balance during movement
• Monitor changes in mobility over time
• Support clinical decision-making and progression of rehabilitation
Unlike isolated gait speed tests, the TUG reflects real-world functional demands, including transitional movements and turning.
3. Constructs Measured
The TUG assesses a composite of functional constructs:
• Lower limb strength (sit-to-stand, stand-to-sit)
• Dynamic balance
• Gait speed and stability
• Turning ability
• Motor planning and coordination
The TUG does not isolate impairments; rather, it provides a global functional mobility index, which must be interpreted alongside impairment-level assessments.
4. Indications and Patient Populations
The TUG is appropriate for use in:
• Stroke and other neurological conditions
• Parkinson’s disease
• Geriatric rehabilitation
• Orthopaedic and post-surgical patients
• ICU step-down and acute care (medically stable patients)
• Community-dwelling older adults
• Vestibular and balance rehabilitation
Patient Prerequisites
The patient should be able to:
• Stand up from a chair (with or without armrests)
• Walk at least 3 meters (with or without an assistive device)
• Follow simple instructions
The test may be inappropriate in:
• Non-ambulatory patients
• Medically unstable patients
• Severe cognitive or behavioral impairment
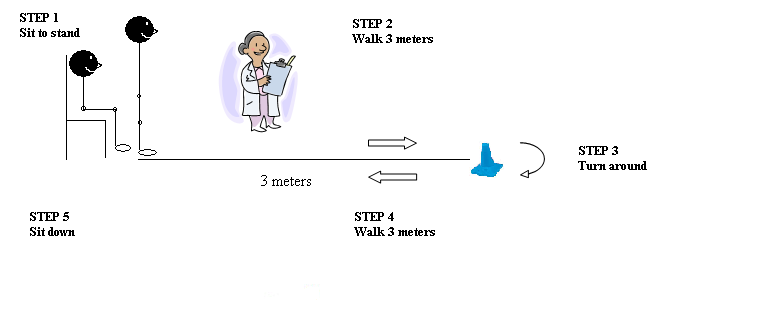
5. Description of the Tool
The Timed Up and Go Test measures the time (in seconds) required for a patient to:
- Stand up from a standard chair
- Walk 3 meters
- Turn around
- Walk back to the chair
- Sit down
The total time reflects overall functional mobility and balance.
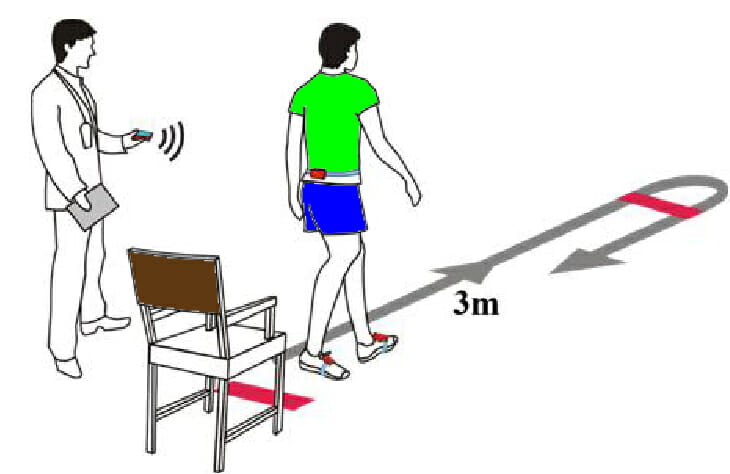
6. Standardized Test Setup
Equipment Required
• Standard chair (seat height ~45 cm)
• Armrests (recommended for standardization)
• Measuring tape (3 meters)
• Stopwatch
• Flat, unobstructed walkway
Environment
• Quiet, well-lit area
• Non-slip floor
• Clear turning point marked on the floor
Standardization of setup is essential to ensure reliable reassessment.
7. Step-by-Step Administration Procedure
Step 1: Patient Positioning
• Patient sits with back against the chair
• Arms resting on armrests
• Feet flat on the floor
• Assistive device positioned within reach (if used)
Step 2: Standardized Instructions
Use the following standardized command:
“When I say ‘go,’ please stand up from the chair, walk at a comfortable and safe speed to the line on the floor, turn around, walk back to the chair, and sit down again.”
Clarify:
• “Walk at your normal pace”
• “Use your usual walking aid if needed”
Step 3: Timing the Test
• Start timing on the word “Go”
• Stop timing when the patient’s back contacts the chair after sitting
Step 4: Safety Monitoring
• Walk beside the patient if fall risk is present
• Do not physically assist unless required for safety
• If assistance is required, document this clearly
Step 5: Recording the Result
Document:
• Time in seconds
• Use of assistive device
• Any deviations (loss of balance, hesitations)
Example:
“TUG: 18.4 seconds, performed with quad cane, unsteady turning noted.”
8. Correct Performance and Common Errors
Correct Practice
• Use the same chair and distance at each reassessment
• Provide identical instructions every time
• Allow one practice trial if needed
Common Errors to Avoid
• Timing from first foot movement instead of “Go”
• Stopping the timer before the patient is fully seated
• Changing walking distance
• Allowing inconsistent assistance
9. Interpretation of TUG Scores
General Reference Values (Adults)
• <10 seconds – Normal mobility
• 10–13.5 seconds – Independent, low fall risk
• >13.5 seconds – Increased fall risk
• >20 seconds – Significant mobility impairment
• >30 seconds – Dependent mobility
These values should be interpreted within the clinical context.
10. Reliability of the TUG
Test–Retest Reliability
• Intraclass Correlation Coefficient (ICC): 0.97–0.99
• Demonstrates excellent stability across neurological and geriatric populations
Inter-Rater Reliability
• ICC ≈ 0.98
• High agreement between different examiners when standardized instructions are used
Clinical implication:
Changes in TUG time are highly likely to reflect true functional change.
11. Validity of the TUG
Construct Validity
The TUG shows strong correlations with:
• Gait speed
• Berg Balance Scale
• Functional mobility measures
Correlation coefficients commonly range from 0.61 to 0.81.
Predictive Validity (Fall Risk)
• A TUG time >13.5 seconds is associated with increased fall risk in community-dwelling older adults.
12. Responsiveness and MCID
Responsiveness
The TUG is responsive to:
• Balance training
• Strengthening interventions
• Task-specific gait training
Minimal Clinically Important Difference (MCID)
Reported MCID values vary by population:
• Older adults: ≈3 seconds
• Stroke survivors: ≈2–3 seconds
Clinical interpretation:
A reduction exceeding these values represents meaningful functional improvement.
13. Clinical Decision-Making Using the TUG
TUG results guide:
• Fall risk stratification
• Need for assistive devices
• Balance and gait training intensity
• Discharge readiness
• Community ambulation safety
Examples:
• TUG >20 sec → prioritize balance and transfer training
• Improving TUG with stable NPRS → progress functional tasks
• Plateauing TUG → reassess impairments and strategy
14. SOAP-Based Documentation Example
S:
Patient reports difficulty standing and walking independently.
O:
TUG: 19.2 seconds using single-point cane; slow turning observed.
A:
Impaired functional mobility and increased fall risk.
P:
Initiate sit-to-stand strengthening, dynamic balance, and gait training. Reassess TUG in 2 weeks.
15. Reassessment and Outcome Tracking
Recommended reassessment:
• Every 1–2 weeks in active rehabilitation
• At discharge
• During functional milestone reviews
The TUG should be paired with:
• Balance scales
• Strength assessments
• ADL measures
16. Advantages and Limitations
Advantages
• Quick (<2 minutes)
• Minimal equipment
• Excellent reliability and validity
• Reflects real-life functional mobility
Limitations
• Does not isolate specific impairments
• Influenced by cognition and motivation
• Ceiling effect in very high-functioning individuals
17. Key Clinical Takeaways
• The TUG is a core functional mobility and fall-risk screening tool
• Demonstrates excellent reliability (ICC up to 0.99)
• Valid predictor of functional decline and falls
• MCID ≈ 2–3 seconds depending on population
• Best used alongside balance and strength measures
18. Key Literature References
- Podsiadlo D, Richardson S. The Timed “Up & Go”: A test of basic functional mobility for frail elderly persons. Journal of the American Geriatrics Society. 1991;39(2):142–148.
- Shumway-Cook A, Brauer S, Woollacott M. Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Physical Therapy. 2000;80(9):896–903.
- Steffen TM, Hacker TA, Mollinger L. Age- and gender-related test performance in community-dwelling elderly people: Six-minute walk test, Berg Balance Scale, Timed Up & Go Test, and gait speeds. Physical Therapy. 2002;82(2):128–137.
- Flansbjer UB, Holmbäck AM, Downham D, Patten C, Lexell J. Reliability of gait performance tests in men and women with hemiparesis after stroke. Journal of Rehabilitation Medicine. 2005;37(2):75–82.
- Bohannon RW, Schaubert KL. Long-term reliability of the Timed Up-and-Go test among community-dwelling elders. Journal of Physical Therapy Science. 2005;17(2):93–96.