Introduction
Early mobilization in the Intensive Care Unit (ICU) represents a paradigm shift from traditional bed-rest–focused critical care toward proactive, function-oriented rehabilitation. It refers to the initiation of physical activity—ranging from passive movements to ambulation—at the earliest physiologically safe point during critical illness. The primary objective is to prevent or attenuate the profound neuromuscular, cardiopulmonary, cognitive, and functional impairments associated with prolonged immobilization and critical illness.
For physiotherapists, ICU early mobilization is a high-level clinical practice domain that demands advanced clinical reasoning, deep understanding of pathophysiology, vigilant risk assessment, and close interprofessional collaboration. This article presents a comprehensive, evidence-informed, and practice-oriented overview of ICU early mobilization principles, with emphasis on safety, decision-making, progression, and outcome optimization.
Rationale for Early Mobilization in the ICU
Prolonged immobilization during critical illness leads to rapid and severe physiological deterioration. Within the first week of ICU admission, patients may experience significant skeletal muscle atrophy, ICU-acquired weakness (ICU-AW), reduced aerobic capacity, joint stiffness, impaired ventilation–perfusion matching, delirium, and long-term functional disability.
Early mobilization addresses these consequences by:
- Preserving muscle mass and neuromuscular integrity
- Improving respiratory mechanics and secretion clearance
- Enhancing cardiovascular conditioning and orthostatic tolerance
- Reducing delirium and improving cognitive outcomes
- Shortening duration of mechanical ventilation and ICU length of stay
- Improving long-term functional independence and quality of life
The principle underpinning early mobilization is that immobility itself is a modifiable iatrogenic harm.
Conceptual Framework of ICU Early Mobilization
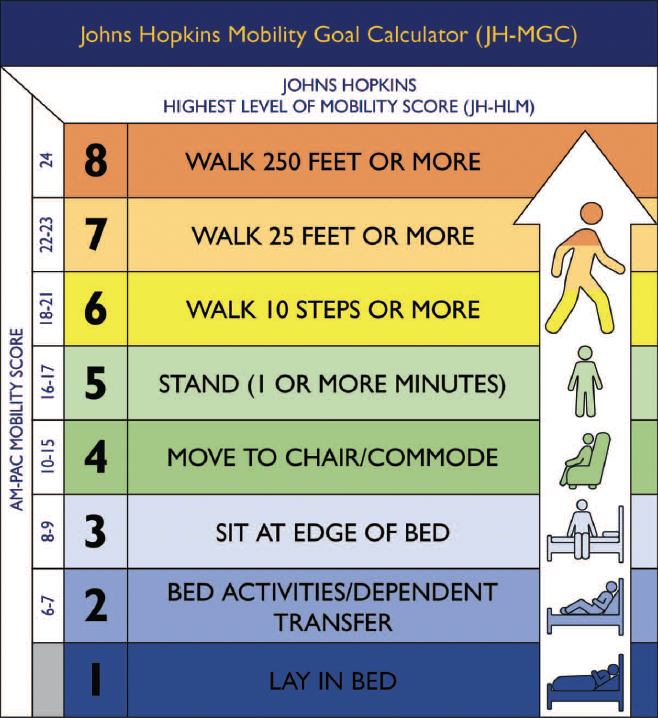


ICU early mobilization is best understood as a continuum rather than a binary intervention. It progresses from low-intensity, low-demand activities to higher-level functional tasks as physiological reserve and neurological status improve.
This continuum typically includes:
- Passive range of motion and positioning
- Active-assisted and active exercises in bed
- Bed mobility and sitting
- Edge-of-bed activities
- Sit-to-stand transfers
- Marching in place
- Ambulation with or without assistive devices
Progression is individualized, non-linear, and responsive to daily fluctuations in clinical status.
Core Principles of ICU Early Mobilization
1. Medical and Physiological Stability First
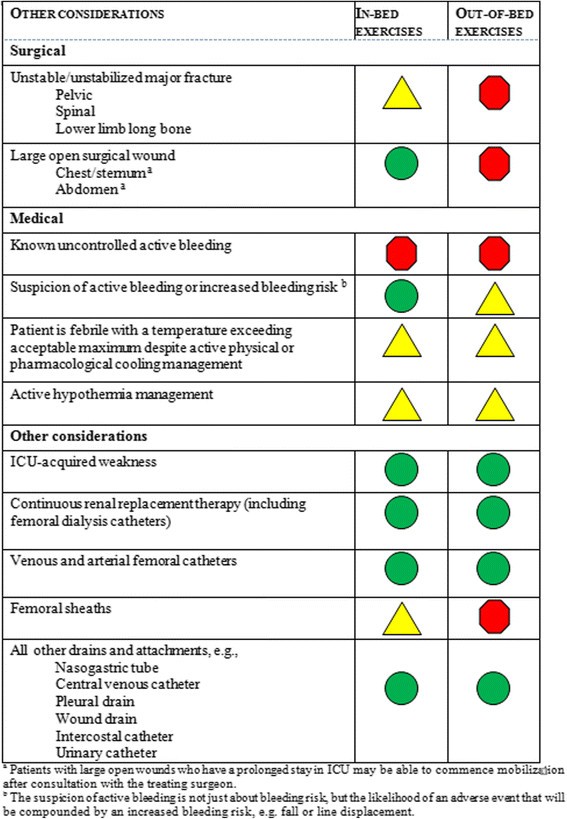
Early mobilization does not imply mobilizing all patients immediately. The foundational principle is physiological stability. Mobilization is initiated only when the patient meets defined safety criteria related to cardiovascular, respiratory, neurological, and metabolic status.
Key considerations include:
- Hemodynamic stability with minimal or stable vasoactive support
- Acceptable oxygenation and ventilatory parameters
- Absence of uncontrolled arrhythmias or active myocardial ischemia
- Stable neurological status without raised intracranial pressure
- Adequate metabolic and hematological parameters
Clinical reasoning must prioritize risk–benefit analysis over protocol rigidity.
2. Safety-Driven, Criteria-Based Decision Making

Early mobilization must be governed by explicit inclusion, exclusion, and termination criteria. Safety is dynamic and must be reassessed before, during, and after each session.
Common termination indicators include:
- Sudden drop or excessive rise in heart rate or blood pressure
- Oxygen desaturation beyond acceptable limits
- Increased work of breathing or ventilator asynchrony
- Patient distress, agitation, or reduced responsiveness
- Equipment compromise (lines, tubes, catheters)
The physiotherapist bears primary responsibility for session-level safety decisions.
3. Individualization Over Standardization
Although mobility protocols provide structure, early mobilization must be tailored to:
- Diagnosis and severity of illness
- Baseline functional status and frailty
- Sedation level and delirium risk
- Mechanical ventilation mode and airway security
- Patient goals and tolerance
Two patients with identical diagnoses may require entirely different mobilization strategies. Individualized clinical reasoning is essential.
4. Interprofessional Collaboration


Early mobilization is a team-based intervention. Effective programs depend on seamless coordination among physiotherapists, intensivists, nurses, respiratory therapists, and support staff.
Key collaborative elements include:
- Daily mobility goal setting during ICU rounds
- Sedation minimization and coordination with nursing care
- Ventilator management adjustments for mobilization
- Clear role delineation and communication during sessions
Physiotherapists often function as mobility leaders within the ICU team.
5. Sedation, Delirium, and Wakefulness Management
Excessive sedation is a major barrier to early mobilization. Mobilization is most effective when integrated with:
- Sedation minimization strategies
- Daily sedation interruption where appropriate
- Delirium screening and management
- Promotion of sleep–wake cycle normalization
Mobilization itself contributes to delirium prevention, creating a positive feedback loop.
6. Functional, Task-Oriented Approach


Early mobilization should prioritize functional tasks over isolated exercises. Task-oriented activities promote neural activation, postural control, and real-world relevance.
Examples include:
- Rolling and bed mobility
- Sitting balance with functional reaching
- Sit-to-stand repetitions
- Weight shifting and stepping
- Ambulation with appropriate support
Function-focused mobilization enhances carryover to post-ICU recovery.
7. Progressive Loading and Dose Regulation
Mobilization follows fundamental rehabilitation principles of overload, specificity, and progression. However, dosage must be conservative and adaptable.
Key dosage variables include:
- Frequency (often daily or twice daily)
- Intensity (perceived exertion, physiological response)
- Duration (short, repeated bouts preferred)
- Complexity (single-task to dual-task activities)
Fatigue and delayed physiological responses are closely monitored.
Special Considerations in Mechanically Ventilated Patients


Mechanical ventilation is not a contraindication to mobilization. Patients can safely participate in sitting, standing, and even ambulation when airway security and ventilator management are optimized.
Critical considerations include:
- Secure fixation of endotracheal or tracheostomy tubes
- Adequate ventilator tubing length and mobility-friendly circuits
- Monitoring of ventilator synchrony
- Close collaboration with respiratory therapists
Mobilizing ventilated patients requires advanced skill but yields substantial benefits.
Clinical Reasoning in ICU Early Mobilization
Clinical reasoning is central to ICU mobilization decisions. Physiotherapists continuously integrate:
- Real-time physiological data
- Patient responsiveness and fatigue
- Risk of adverse events
- Expected functional benefit
Decision-making is iterative, with constant reassessment and modification. Expert clinicians balance caution with therapeutic challenge.
Outcome Measures and Monitoring
Outcome assessment guides progression and program evaluation. Common measures include:
- Muscle strength grading
- ICU Mobility Scale
- Functional Status Score for the ICU
- Duration of mechanical ventilation
- ICU and hospital length of stay
Functional outcomes, not just physiological stability, define success.
Barriers to ICU Early Mobilization
Despite strong evidence, implementation challenges persist:
- Staffing limitations
- Cultural resistance to mobilizing critically ill patients
- Fear of adverse events
- Inadequate training or protocols
- Equipment constraints
Overcoming these barriers requires leadership, education, and institutional commitment.
Future Directions
Advances in ICU rehabilitation include:
- Integration of mobility into ICU quality indicators
- Use of technology-assisted mobilization
- Enhanced training in critical care physiotherapy
- Long-term follow-up of ICU survivors
Early mobilization is increasingly recognized as a standard of high-quality critical care.
Conclusion
ICU early mobilization is a safe, effective, and essential component of modern critical care rehabilitation. It mitigates the devastating consequences of immobilization, accelerates recovery, and improves long-term functional outcomes. Successful implementation depends on rigorous clinical reasoning, safety-driven decision-making, interprofessional collaboration, and a functional, patient-centered approach. For physiotherapists, early mobilization is not an adjunct to ICU care—it is a core responsibility.
Key References
Schweickert WD, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients. Lancet. 2009.
Needham DM, et al. Early physical medicine and rehabilitation for patients with acute respiratory failure. Arch Phys Med Rehabil. 2010.
Adler J, Malone D. Early mobilization in the ICU: a systematic review. Cardiopulmonary Physical Therapy Journal. 2012.
Fan E, et al. Physical complications in ICU survivors. Intensive Care Medicine. 2014.
Stiller K. Physiotherapy in intensive care: an updated systematic review. Chest. 2013.