Outcome measures are fundamental to neurological rehabilitation. They provide objective, standardized methods to quantify impairments, activity limitations, participation restrictions, and quality of life in individuals with neurological disorders. In physiotherapy practice, outcome measures serve multiple critical purposes: guiding clinical reasoning, informing goal setting, monitoring progress, evaluating treatment effectiveness, supporting communication within the multidisciplinary team, and demonstrating the value of rehabilitation to patients, institutions, and health systems.
Neurological rehabilitation is characterized by complexity, heterogeneity, and long recovery trajectories. Spontaneous recovery, neuroplastic changes, compensatory strategies, and contextual factors interact in ways that are not always linear or predictable. Consequently, reliance on subjective impression alone is insufficient. Carefully selected, valid, and responsive outcome measures are essential to ensure evidence-based, patient-centered, and accountable care.
This article provides a comprehensive and structured overview of outcome measures in neurological rehabilitation, with emphasis on conceptual frameworks, classification, psychometric properties, condition-specific tools, and practical clinical application.
Conceptual Framework for Outcome Measurement

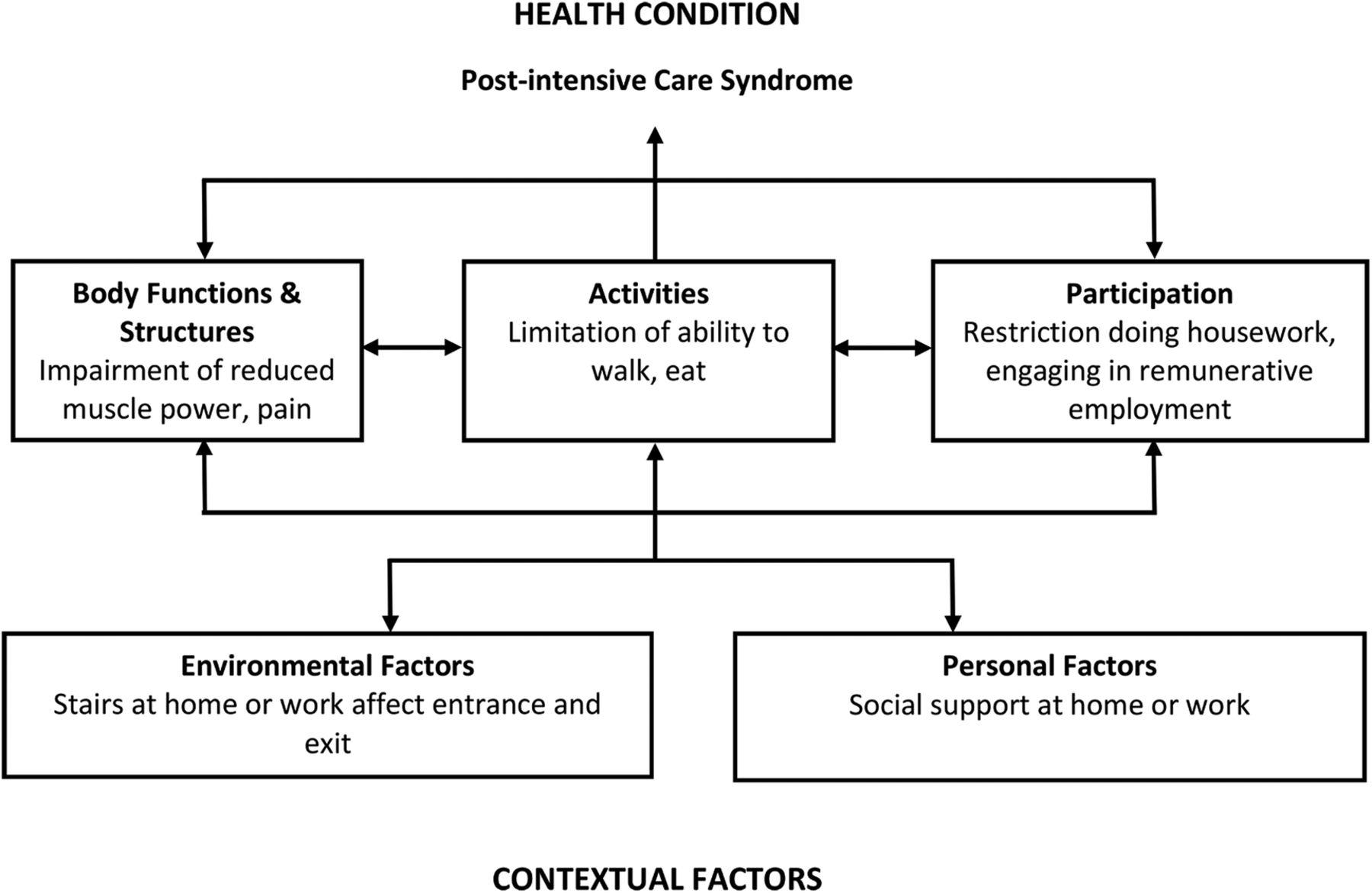
The International Classification of Functioning, Disability and Health (ICF) framework provides the most widely accepted conceptual foundation for outcome measurement in neurological rehabilitation. It shifts the focus from disease-centered outcomes to a holistic view of functioning.
Within this framework, outcome measures are broadly classified into:
- Body structure and function (impairment-level measures)
- Activity-level measures
- Participation-level measures
- Contextual and quality-of-life measures
Comprehensive neurological rehabilitation requires assessment across multiple ICF domains, as improvement at one level does not automatically translate to gains at another.
Key Psychometric Properties of Outcome Measures
Before selecting any outcome measure, physiotherapists must consider its psychometric robustness. The clinical utility of a measure depends not only on what it assesses, but on how well it measures it.
Validity refers to whether the instrument measures what it claims to measure. This includes content validity, construct validity, and criterion validity.
Reliability reflects the consistency of measurements across time, raters, and testing conditions.
Responsiveness indicates the ability of a measure to detect clinically meaningful change over time.
Minimal Clinically Important Difference (MCID) represents the smallest change perceived as beneficial by the patient or clinically meaningful by the therapist.
Feasibility and interpretability are equally important, particularly in busy clinical environments and in patients with cognitive, communication, or fatigue limitations.
Impairment-Level Outcome Measures


Impairment-level measures quantify deficits in body structure and function, such as muscle strength, tone, sensation, coordination, and postural control.
Common domains and examples include:
- Muscle strength assessed through manual muscle testing or dynamometry
- Muscle tone and spasticity assessed through clinical scales and biomechanical measures
- Selective motor control and coordination assessed through limb-specific tasks
- Balance and postural control assessed through static and dynamic balance tests
- Sensation and proprioception assessed through standardized sensory testing
While impairment-level measures are important for understanding underlying deficits and guiding intervention selection, they should not be used in isolation, as they do not fully capture functional performance.
Activity-Level Outcome Measures

Activity-level measures assess a patient’s ability to perform specific tasks or actions. These measures are central to physiotherapy practice, as they reflect functional capability and independence.
Key activity domains include:
- Mobility and transfers
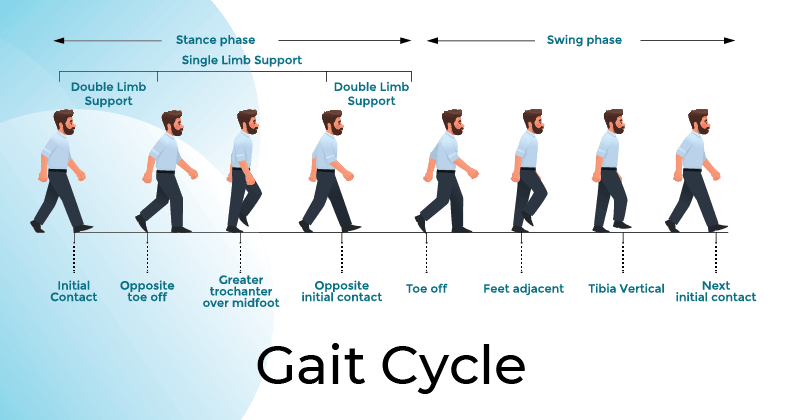
- Gait and locomotion
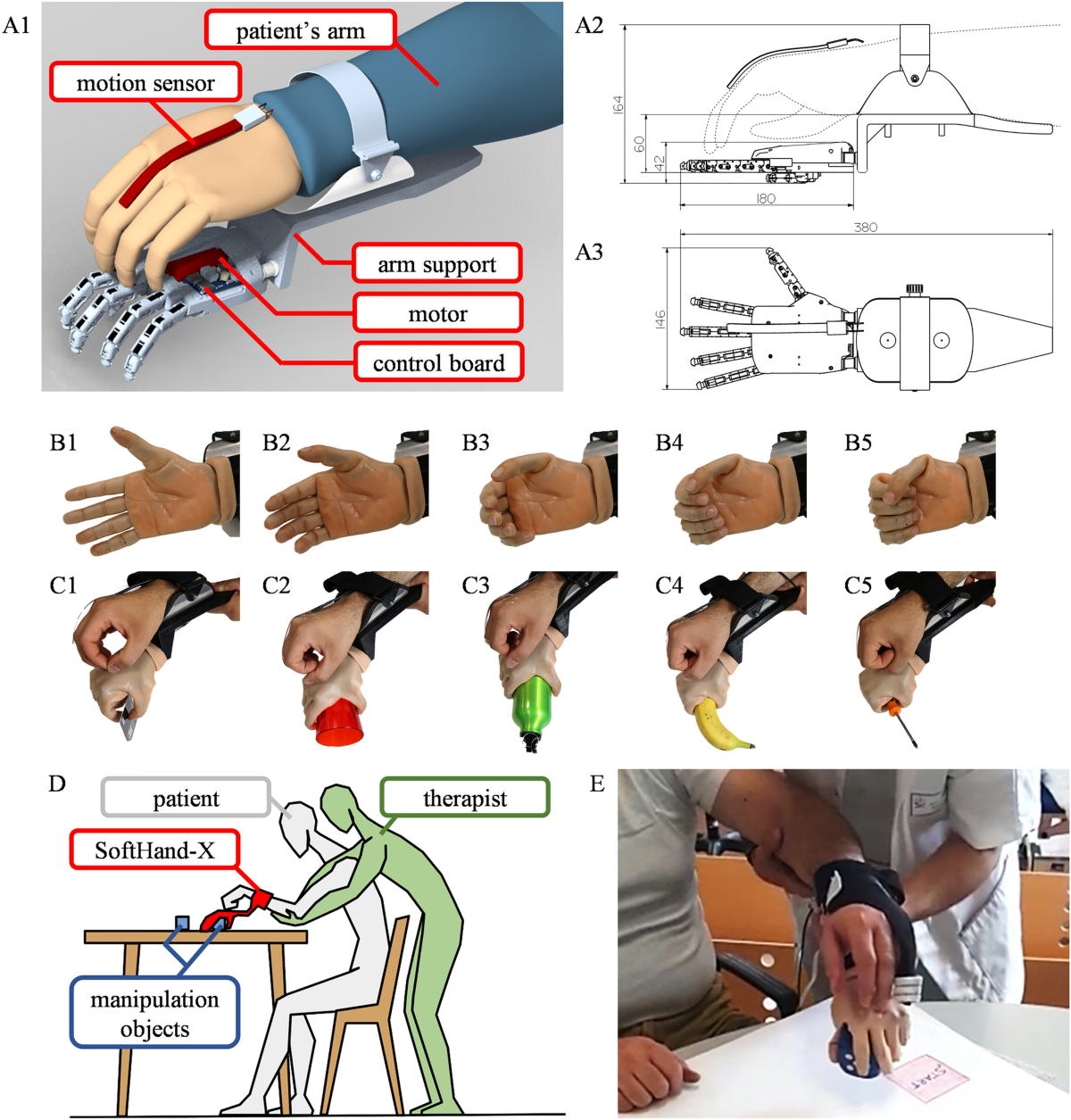
- Upper limb function and dexterity
- Balance during functional tasks
Activity-level outcome measures are particularly valuable for goal setting, progression of therapy, and discharge planning. They often demonstrate stronger responsiveness to rehabilitation interventions than impairment-level measures.
Participation-Level and Quality-of-Life Measures

Participation-level measures evaluate involvement in life situations, such as work, social roles, leisure, and community engagement. These outcomes are often most meaningful to patients and families.
Quality-of-life measures capture the broader impact of neurological conditions on physical, emotional, cognitive, and social well-being.
Key considerations include:
- Alignment with patient priorities
- Cultural and contextual relevance
- Sensitivity to long-term change
Although participation and quality-of-life outcomes may change more slowly than impairment or activity measures, they are essential for evaluating long-term rehabilitation success.
Condition-Specific Outcome Measures in Neurological Rehabilitation

4
Neurological rehabilitation encompasses diverse conditions, each with distinct recovery patterns and outcome priorities.
Stroke rehabilitation emphasizes motor recovery, balance, gait, upper limb function, and independence in daily activities.
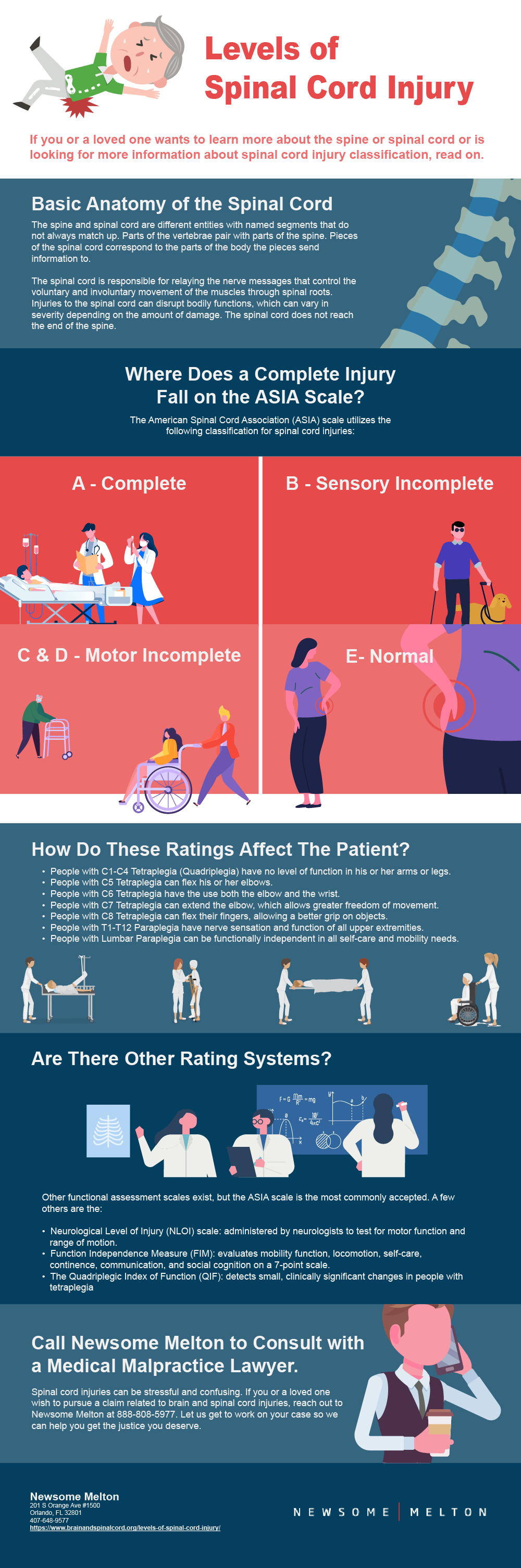
Spinal cord injury rehabilitation focuses on neurological level, motor and sensory recovery, functional independence, wheelchair skills, and participation.
Traumatic brain injury rehabilitation prioritizes functional mobility, balance, cognition–motor interaction, and community reintegration.
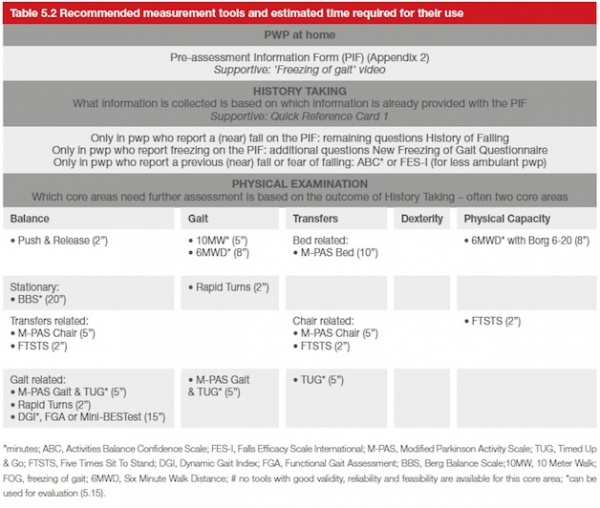
Parkinsonian syndromes emphasize gait, balance, postural stability, and functional mobility under dual-task conditions.
Condition-specific measures enhance sensitivity and clinical relevance but should be complemented by generic measures to allow comparison across populations and settings.
Outcome Measures Across the Rehabilitation Continuum

Outcome measurement strategies must adapt across phases of recovery.
- Acute phase: focus on impairments, consciousness, basic mobility, and prevention of secondary complications
- Subacute phase: emphasis on functional gains, task performance, and responsiveness to therapy
- Chronic phase: focus on participation, quality of life, self-management, and long-term adaptation
Timing and frequency of outcome measurement are as important as tool selection.
Clinical Reasoning in Outcome Measure Selection
Outcome measures should never be chosen arbitrarily. Selection requires structured clinical reasoning based on:
- Patient diagnosis and severity
- Stage of recovery
- Cognitive and communication abilities
- Goals of intervention
- Sensitivity to expected change
- Clinical setting and resources
Using too many measures increases burden without adding value, while using too few risks missing meaningful change.
Documentation, Audit, and Research Applications
Outcome measures provide the foundation for:
- Transparent clinical documentation
- Communication within multidisciplinary teams
- Quality assurance and service evaluation
- Clinical audit and benchmarking
- Research and evidence generation
In neurological rehabilitation, standardized outcome measurement bridges clinical practice and research, strengthening professional credibility and advancing the discipline.
Challenges and Limitations
Despite their importance, outcome measures in neurological rehabilitation face challenges:
- Ceiling and floor effects
- Limited responsiveness in severely impaired patients
- Cultural and linguistic barriers
- Time constraints in clinical settings
- Overemphasis on numerical change without clinical context
Expert clinicians interpret outcomes within the broader clinical picture rather than relying solely on scores.
Future Directions in Outcome Measurement
Emerging trends include:
- Technology-assisted outcome measurement
- Wearable sensors and digital biomarkers
- Ecologically valid, real-world activity monitoring
- Integration of patient-reported outcomes
- Longitudinal tracking across care settings
These advances will complement, not replace, clinician-administered measures and professional judgment.
Conclusion
Outcome measures are indispensable tools in neurological rehabilitation. They enable objective evaluation of impairment, function, participation, and quality of life, supporting evidence-based and patient-centered physiotherapy practice. Optimal use of outcome measures requires sound clinical reasoning, understanding of psychometric properties, and alignment with patient goals and rehabilitation phase. When used judiciously, outcome measures enhance clinical decision-making, improve communication, and ultimately contribute to better long-term outcomes for individuals with neurological conditions.
Key References
World Health Organization. International Classification of Functioning, Disability and Health. 2001.
Jette AM, Haley SM. Contemporary measurement techniques for rehabilitation outcomes. Rehabilitation Psychology.
Lang CE, et al. Measurement of upper-extremity function in neurological rehabilitation. Neurorehabilitation and Neural Repair.
Salter K, et al. Outcome measures in stroke rehabilitation. Stroke.
van Peppen RP, et al. Clinical relevance and responsiveness of outcome measures in neurological physiotherapy.