
ICU MOBILITY SCALE (IMS)
A Comprehensive Clinical Guide for Physiotherapists
1. Introduction and Clinical Importance
Early and progressive mobilization in the Intensive Care Unit (ICU) is now a cornerstone of modern critical care rehabilitation. Prolonged immobility in critically ill patients contributes to ICU-acquired weakness, delirium, prolonged ventilation, functional decline, and increased length of stay. To implement early mobilization safely and consistently, clinicians require a simple, standardized, and reproducible mobility classification tool.
The ICU Mobility Scale (IMS) was developed specifically to quantify the highest level of mobility achieved by a patient in the ICU on a given day. It provides a shared language for physiotherapists, intensivists, nurses, and the multidisciplinary team to track mobility progression, set daily goals, and evaluate rehabilitation outcomes.
Within a physiotherapy intranet, the IMS should be considered a mandatory acute-care outcome and communication tool, particularly for ICU, HDU, and step-down units.
2. Purpose of the ICU Mobility Scale
The ICU Mobility Scale is designed to:
• Quantify current functional mobility status in ICU patients
• Track daily mobility progression
• Support early mobilization protocols
• Facilitate interdisciplinary communication
• Provide objective data for quality improvement and audit
The IMS captures what the patient actually achieved, not their potential capacity.
3. Construct Measured
Primary construct:
• Highest level of mobility activity performed safely during a session or day
The IMS integrates:
• Consciousness and cooperation
• Postural control
• Strength and endurance
• Cardiopulmonary stability
• Assistance and device requirements
It does not measure:
• Muscle strength in isolation
• Balance quality
• Exercise intensity
These domains should be assessed separately when needed.
4. Indications and Patient Populations
The IMS is appropriate for:
• Mechanically ventilated ICU patients
• Post-surgical ICU admissions
• Medical ICU patients (sepsis, ARDS, cardiac conditions)
• Neurological ICU patients
• ICU step-down and HDU patients
It is applicable from deeply sedated states to independent ambulation.
5. Description of the Tool
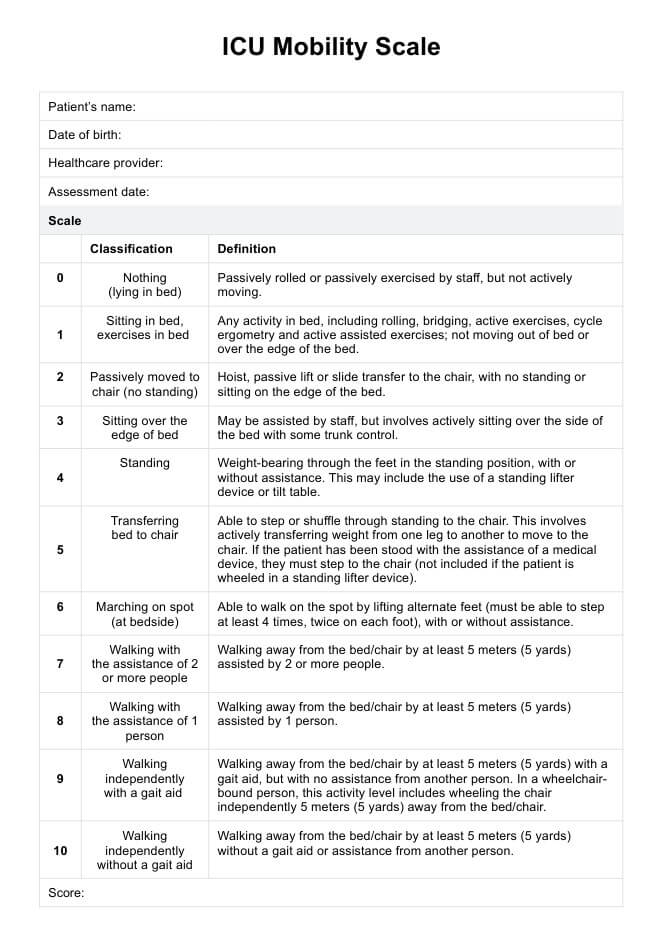
The ICU Mobility Scale is an 11-point ordinal scale (0–10) that classifies mobility based on the highest level achieved.
ICU Mobility Scale Levels
• 0 – Nothing (lying in bed, passive movements only)
• 1 – Sitting in bed, exercises in bed
• 2 – Passively moved to chair (hoist)
• 3 – Sitting over edge of bed
• 4 – Standing
• 5 – Transferring bed to chair
• 6 – Marching on the spot (bedside stepping)
• 7 – Walking with assistance of ≥2 people
• 8 – Walking with assistance of 1 person
• 9 – Walking independently with a gait aid
• 10 – Walking independently without a gait aid
The score reflects the single highest activity completed safely.
6. Equipment and Environment
Equipment (as required)
• ICU bed with adjustable height
• Chair or recliner
• Hoist (for passive transfers)
• Gait belt
• Walking aids (walker, cane)
• Monitoring devices (ECG, SpO₂, BP)
Environment
• ICU bedside or corridor
• Clear space for transfers and ambulation
• Adequate staffing for safety
7. Step-by-Step Administration Procedure
Step 1: Pre-Mobilization Safety Screening
Before attempting mobilization, confirm:
• Hemodynamic stability
• Acceptable oxygenation and ventilator settings
• Absence of unstable lines or contraindications
• Adequate level of alertness and cooperation
Safety screening is mandatory prior to IMS scoring.
Step 2: Determine Starting Level
Based on:
• Consciousness
• Previous IMS score
• Medical stability
Begin at a safe and achievable level.
Step 3: Mobilization Attempt
Progressively attempt activities:
• Bed mobility
• Sitting
• Standing
• Transfers
• Ambulation
Stop progression if:
• Patient becomes unstable
• Excessive fatigue or distress occurs
• Safety is compromised
Step 4: Assign IMS Score
Record the highest level successfully completed during the session or day.
Key principle:
If assistance or safety limitations prevent progression, do not score higher levels.
Step 5: Documentation
Document:
• IMS score
• Level of assistance
• Devices used
• Patient tolerance and adverse events
Example:
“IMS = 5; transferred bed to chair with assistance of two staff, stable vitals.”
8. Correct Scoring and Common Errors
Correct Practice
• Score actual achieved mobility, not planned goals
• Use the highest level completed safely
• Maintain consistency across sessions
Common Errors
• Scoring potential instead of performance
• Averaging multiple activities
• Ignoring safety interruptions
• Confusing marching in place with walking
9. Interpretation of IMS Scores
Clinical Meaning
• IMS 0–2: Severe immobility, bed-based care
• IMS 3–4: Early upright tolerance
• IMS 5–6: Functional transfers and pre-gait activity
• IMS 7–10: Ambulatory stages
Daily upward progression reflects successful early rehabilitation.
10. Reliability of the ICU Mobility Scale
Inter-Rater Reliability
• Reported ICC values: 0.90–0.95
• Excellent agreement among ICU clinicians
Test–Retest Reliability
• High stability when patient condition is unchanged
Clinical implication:
IMS provides consistent and reproducible mobility classification across raters.
11. Validity of the ICU Mobility Scale
Construct Validity
• Strong correlation with:
– Physical function at ICU discharge
– Length of ICU stay
– Duration of mechanical ventilation
Correlation coefficients reported between 0.60 and 0.80.
Predictive Validity
• Higher IMS scores are associated with:
– Earlier ICU discharge
– Improved functional outcomes
– Reduced hospital length of stay
12. Responsiveness and Clinically Meaningful Change
Responsiveness
The IMS is highly responsive to:
• Daily physiotherapy input
• Early mobilization protocols
• Sedation minimization strategies
Clinically Meaningful Change
• An improvement of ≥1 IMS level is clinically meaningful
• Sustained progression across days indicates functional recovery
13. Clinical Decision-Making Using IMS
IMS scores guide:
• Daily mobilization goals
• Staffing and equipment requirements
• Progression from bed-based to upright activity
• Communication during ward rounds
Examples:
• IMS 0–1 → focus on positioning and in-bed exercise
• IMS 3–4 → emphasize sitting balance and standing tolerance
• IMS ≥7 → progress ambulation distance and independence
14. SOAP-Based Documentation Example
S:
Patient reports dizziness on sitting upright.
O:
IMS: 3; able to sit at edge of bed with assistance, vitals stable.
A:
Limited upright tolerance but appropriate for early mobilization.
P:
Progress sitting endurance and attempt standing next session. Reassess IMS daily.
15. Reassessment and Outcome Tracking
Recommended use:
• Daily IMS scoring in ICU
• Track trends rather than single scores
• Use alongside sedation, delirium, and strength measures
IMS is ideal for daily mobility dashboards in ICU settings.
16. Advantages and Limitations
Advantages
• ICU-specific and practical
• Quick to administer
• Excellent reliability and validity
• Supports early mobilization culture
Limitations
• Ordinal scale with broad levels
• Does not quantify distance or endurance
• Dependent on staffing and environment
17. Key Clinical Takeaways
• IMS is a core ICU mobility outcome measure
• Captures highest safe mobility achieved
• Demonstrates strong reliability and validity
• A 1-level change is clinically meaningful
• Essential for early mobilization protocols and communication
18. Key Literature References
- Hodgson CL, Bailey M, Bellomo R, et al. A binational multicenter pilot feasibility randomized controlled trial of early goal-directed mobilization in the ICU. Critical Care. 2016;20:81.
- Hodgson CL, Stiller K, Needham DM, et al. Expert consensus and recommendations on safety criteria for active mobilization of mechanically ventilated critically ill adults. Critical Care. 2014;18(6):658.
- Tipping CJ, Bailey MJ, Bellomo R, et al. The ICU Mobility Scale has construct and predictive validity and is responsive: A multicenter observational study. Annals of the American Thoracic Society. 2016;13(6):887–893.
- Schweickert WD, Pohlman MC, Pohlman AS, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients. The Lancet. 2009;373(9678):1874–1882.
- Needham DM, Davidson J, Cohen H, et al. Improving long-term outcomes after discharge from intensive care unit: Report from a stakeholders’ conference. Critical Care Medicine. 2012;40(2):502–509.