
BORG RATING OF PERCEIVED EXERTION (RPE)
A Comprehensive Clinical Guide for Physiotherapists
1. Introduction and Clinical Importance
Safe and effective exercise prescription in physiotherapy requires accurate monitoring of exercise intensity. While heart rate and oxygen consumption provide objective physiological data, they are not always feasible, reliable, or sufficient—particularly in patients taking beta-blockers, those with autonomic dysfunction, or in resource-limited settings.
The Borg Rating of Perceived Exertion (RPE) scale is a validated, patient-reported measure of exercise intensity that reflects the integrated response of the cardiovascular, respiratory, and musculoskeletal systems. It is a cornerstone tool in cardiac, pulmonary, neurological, geriatric, sports, and general rehabilitation, and is recommended by international exercise and rehabilitation guidelines.
Within a physiotherapy intranet, Borg RPE should be treated as a mandatory monitoring tool for aerobic training, endurance exercises, circuit training, and early mobilization.
2. Purpose of the Borg RPE
The Borg RPE is designed to:
• Quantify subjective exercise intensity
• Guide safe exercise prescription and progression
• Monitor patient tolerance and fatigue
• Complement physiological measures (HR, SpO₂, BP)
• Support self-monitoring and patient education
It reflects how hard the exercise feels to the patient, not how hard it appears objectively.
3. Constructs Measured
The Borg RPE captures a global perceptual construct that integrates:
• Breathlessness
• Muscular fatigue
• Cardiovascular strain
• Overall effort
It does not isolate:
• Pain intensity
• Local muscle endurance
• Psychological distress
Separate tools are required for those domains.
4. Borg RPE Scales Used in Physiotherapy
Two versions are commonly used:
A. Borg 6–20 Scale (Original)
• Range: 6 to 20
• Designed to approximate heart rate (RPE × 10 ≈ HR)
B. Modified Borg 0–10 Scale
• Range: 0 to 10
• Easier for patient understanding
• Commonly used in pulmonary and cardiac rehab
Both scales are valid; consistency is essential during reassessment.
5. Indications and Patient Populations
Borg RPE is appropriate for:
• Cardiac rehabilitation
• Pulmonary rehabilitation (COPD, ILD, post-COVID)
• Neurological rehabilitation
• Geriatric populations
• ICU and early mobilization
• Sports and fitness rehabilitation
• Patients on heart-rate-altering medications
It is particularly valuable when:
• HR monitoring is unreliable
• Exercise intensity must be self-regulated
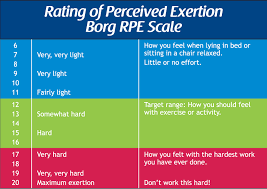
6. Description of the Scale
Borg 6–20 Scale (Selected Anchors)
• 6 – No exertion
• 9 – Very light
• 11 – Light
• 13 – Somewhat hard
• 15 – Hard
• 17 – Very hard
• 19–20 – Extremely hard / maximal
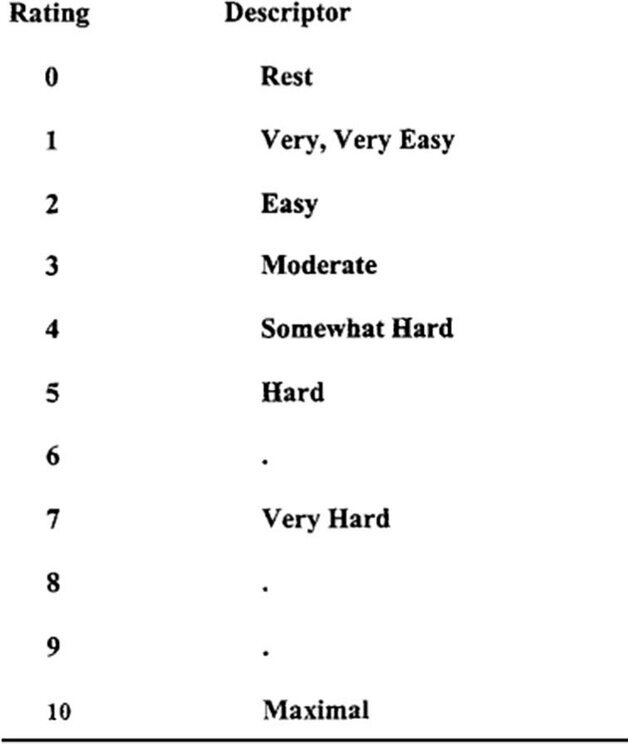
Modified Borg 0–10 Scale
• 0 – Nothing at all
• 2 – Slight
• 4 – Moderate
• 6 – Severe
• 8 – Very severe
• 10 – Maximal
Patients should be familiarized with the verbal descriptors, not just numbers.
7. Step-by-Step Administration Procedure
Step 1: Patient Education
Explain clearly:
“This scale helps you tell me how hard the exercise feels overall—not just your breathing or your legs, but your whole body.”
Ensure understanding before exercise begins.
Step 2: Introduce the Scale Visually
• Show the scale chart
• Read the descriptors aloud
• Confirm the patient understands the anchors
Step 3: Timing of Assessment
Ask for RPE:
• During steady-state exercise
• At peak effort
• Immediately after exercise completion
Avoid asking too frequently, which may disrupt exercise.
Step 4: Standardized Questioning
Use consistent phrasing:
“How hard does this exercise feel to you right now?”
Avoid leading questions such as “Is this hard?”
Step 5: Recording the Score
Document:
• RPE score
• Type of scale used (6–20 or 0–10)
• Exercise modality and intensity
Example:
“RPE: 13/20 during treadmill walking at 3 km/h.”
8. Correct Use and Common Errors
Correct Practice
• Use the same scale consistently
• Combine RPE with objective measures
• Educate patients for accurate self-reporting
Common Errors
• Switching between scales without documentation
• Interpreting RPE as pain
• Ignoring unusually high or low RPE responses
• Using RPE without prior patient education
9. Interpretation of RPE Scores
Exercise Intensity Zones (6–20 Scale)
• 9–11: Light (warm-up, early rehab)
• 12–13: Moderate (aerobic conditioning)
• 14–16: Vigorous (advanced conditioning)
• ≥17: Near-maximal / maximal
Exercise Intensity Zones (0–10 Scale)
• 0–2: Very light
• 3–4: Moderate
• 5–6: Hard
• ≥7: Very hard
10. Reliability of Borg RPE
Test–Retest Reliability
• Reliability coefficients reported: 0.83–0.95
Inter-Individual Reliability
• High consistency when patients are properly educated
Clinical implication:
Borg RPE provides reliable exercise intensity monitoring across sessions and settings.
11. Validity of Borg RPE
Concurrent Validity
• Strong correlation with:
– Heart rate
– Oxygen uptake (VO₂)
– Blood lactate
Correlation coefficients typically range from 0.70 to 0.90.
Construct Validity
• Accurately reflects integrated physiological stress during exercise
This supports its use as a valid surrogate of exercise intensity.
12. Responsiveness and Clinically Meaningful Change
Responsiveness
Borg RPE responds to:
• Training adaptation
• Improved exercise tolerance
• Reduced cardiopulmonary strain
Clinically Meaningful Interpretation
• Lower RPE at the same workload indicates improved fitness
• Higher RPE at lower workload may indicate fatigue or deconditioning
There is no fixed MCID; interpretation is context-dependent.
13. Clinical Decision-Making Using Borg RPE
Borg RPE guides:
• Aerobic exercise prescription
• Intensity progression and regression
• Safety monitoring during training
• Patient self-management strategies
Examples:
• Target RPE 11–13 → moderate aerobic training
• RPE >15 early in session → reduce workload
• Rising RPE with stable vitals → monitor fatigue and pacing
14. SOAP-Based Documentation Example
S:
Patient reports early fatigue during walking exercises.
O:
Borg RPE: 15/20 at 4 minutes of treadmill walking.
A:
Exercise intensity currently exceeds moderate level.
P:
Reduce treadmill speed and target RPE 12–13. Reassess tolerance next session.
15. Reassessment and Outcome Tracking
Borg RPE should be recorded:
• During every aerobic session
• At key intensity changes
• During reassessment sessions
Tracking trends over time provides insight into training adaptation.
16. Advantages and Limitations
Advantages
• Simple and cost-free
• No equipment required
• Valid across diverse populations
• Empowers patient self-monitoring
Limitations
• Subjective and experience-dependent
• Requires patient understanding
• Influenced by mood and motivation
17. Key Clinical Takeaways
• Borg RPE is a core tool for monitoring exercise intensity
• Valid and reliable surrogate of physiological stress
• Essential when HR monitoring is unreliable
• Guides safe and effective exercise prescription
• Should always be combined with clinical judgment
18. Key Literature References
- Borg G. Perceived exertion as an indicator of somatic stress. Scandinavian Journal of Rehabilitation Medicine. 1970;2(2):92–98.
- Borg G. Borg’s Perceived Exertion and Pain Scales. Human Kinetics; 1998.
- Noble BJ, Robertson RJ. Perceived Exertion. Human Kinetics; 1996.
- Chen MJ, Fan X, Moe ST. Criterion-related validity of the Borg ratings of perceived exertion scale in healthy individuals: A meta-analysis. Journal of Sports Sciences. 2002;20(11):873–899.
- American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription. 11th ed. Wolters Kluwer; 2021.