Load, Dosage, and Specificity in Physiotherapy and Rehabilitation Practice
Introduction
Therapeutic exercise is universally acknowledged as the central intervention in physiotherapy and rehabilitation. However, clinical effectiveness is not determined merely by exercise selection, but by how exercises are progressed over time. Inappropriate progression remains one of the most common reasons for treatment failure, symptom recurrence, delayed recovery, and patient dissatisfaction.
Evidence-based progression of therapeutic exercise refers to the systematic, measurable, and individualized advancement of exercise parameters, guided by scientific principles, tissue healing biology, motor learning theories, and ongoing patient response. Progression must be planned rather than intuitive, measured rather than assumed, and individualized rather than protocol-driven alone.
Three interdependent pillars govern therapeutic exercise progression:
- Load – the magnitude of stress applied
- Dosage – the total volume and frequency of exposure
- Specificity – the relevance of the exercise to the desired functional outcome
This article provides a comprehensive exploration of each pillar and demonstrates how they must be integrated through clinical reasoning to achieve safe, effective, and durable rehabilitation outcomes.
Conceptual Foundations of Exercise Progression in Rehabilitation
Why Progression Matters in Physiotherapy
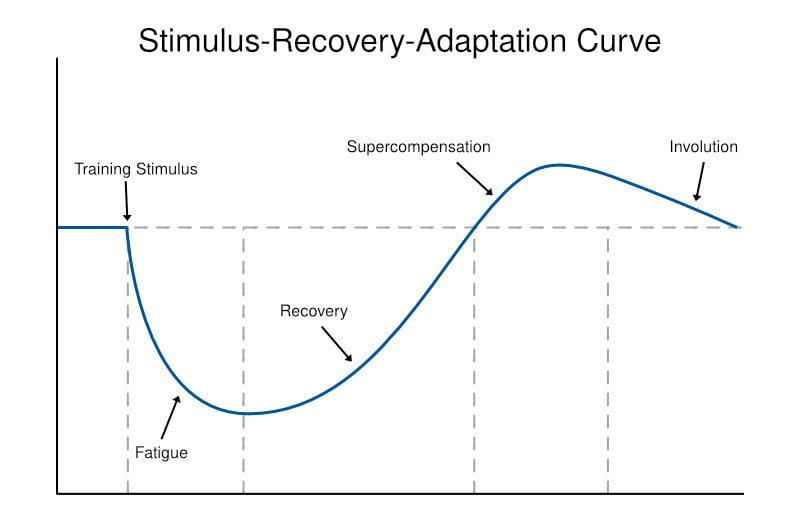
Human tissues and systems adapt only when exposed to sufficient challenge followed by recovery. This principle applies across:
• Musculoskeletal tissues (muscle, tendon, bone)
• Neurological systems (motor cortex, spinal pathways)
• Cardiopulmonary systems (oxygen transport and utilization)
However, rehabilitation differs from fitness training because:
• The starting point is often tissue injury or neurological impairment
• Load tolerance is reduced and asymmetrical
• Pain and fear alter motor output
• Overload can reverse healing rather than promote adaptation
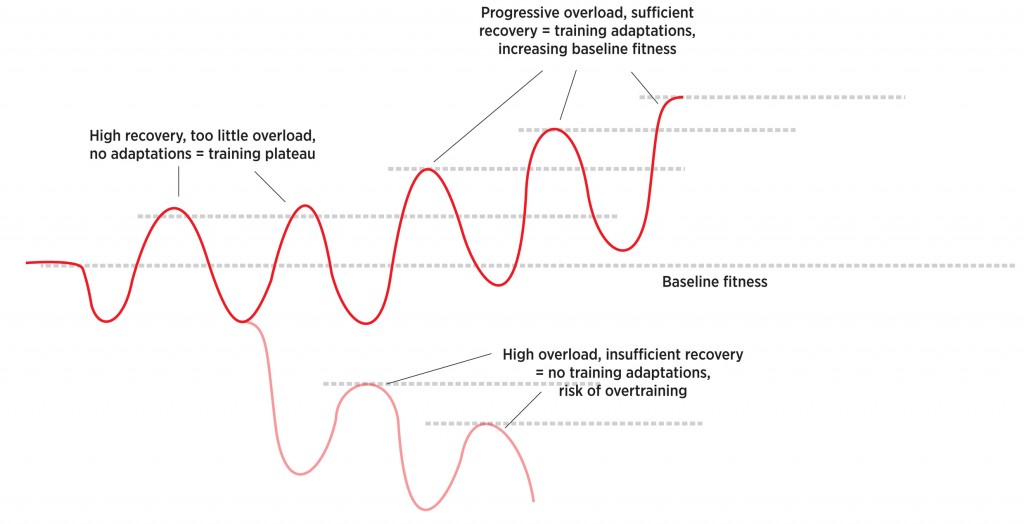
This visual conceptually demonstrates the balance between applied stress and recovery. It helps clinicians understand why both under-loading and over-loading fail to stimulate optimal adaptation, reinforcing the need for graded progression.
Pillar I: Load Progression
Defining Load in a Rehabilitation Context
Load refers to the mechanical, physiological, and neuromuscular demand imposed on the body during exercise.
In rehabilitation, load is not limited to external resistance and may arise from:
• Body weight
• Gravity and posture
• Joint leverage and moment arms
• Speed of movement
• Ground reaction forces
• Cognitive or dual-task demands
Understanding load in this broader sense allows clinicians to progress exercise even when external resistance is contraindicated.
Biological Rationale for Load Progression
Mechanical loading drives adaptation through mechanotransduction, whereby physical forces are converted into cellular signals that stimulate:
• Muscle protein synthesis
• Tendon collagen realignment
• Bone remodeling
• Improved neuromuscular efficiency
Without progressive loading:
• Strength plateaus
• Tendons remain mechanically weak
• Bone density declines
• Functional capacity stagnates
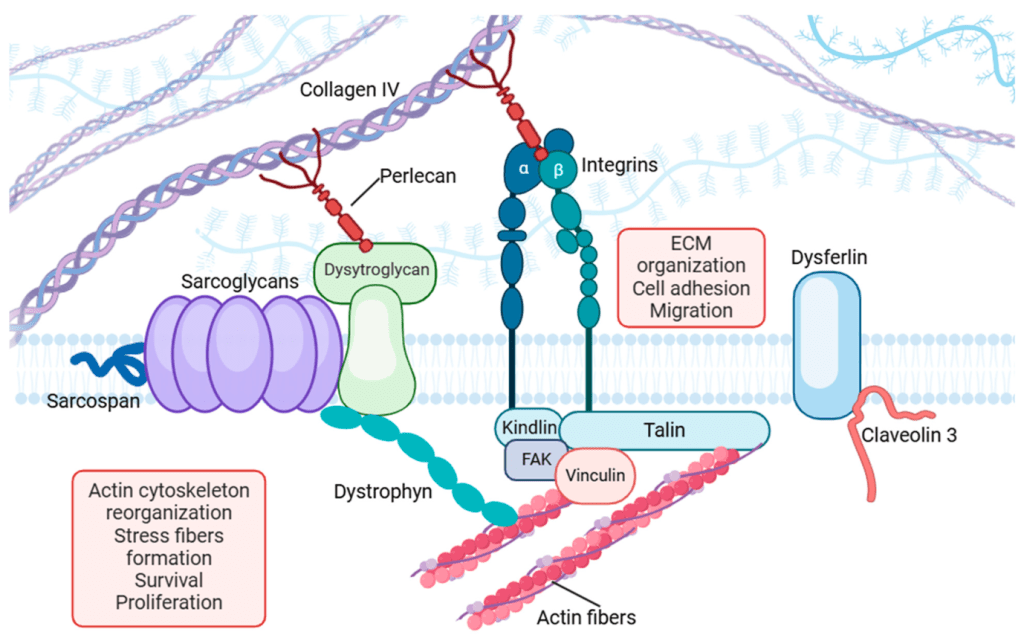
Why this illustration is relevant:
This image set visually links loading to tissue-level adaptation, reinforcing the scientific basis for progressive loading rather than symptom-limited exercise alone.
Clinical Methods of Load Progression
Load can be progressed using multiple strategies:
• Incremental resistance increase
• Lever arm lengthening
• Transition from supported to unsupported postures
• Bilateral to unilateral loading
• Slow to fast movement velocities
• Stable to unstable surfaces
Each method increases demand through different mechanisms and should be selected based on patient tolerance and rehabilitation stage.
Table 1. Common Load Progression Strategies and Clinical Purpose
| Load Progression Method | How Load Increases | Clinical Relevance |
| Resistance increment | Higher force demand | Builds strength safely |
| Lever arm lengthening | Increased joint torque | Useful when weights are limited |
| Postural change | Greater gravitational demand | Improves functional relevance |
| Velocity increase | Higher neuromuscular demand | Prepares for dynamic tasks |
| Environmental challenge | Increased postural control | Enhances real-world readiness |
This table provides a structured clinical decision aid, helping clinicians select load progression strategies based on rehabilitation goals rather than defaulting to weight increases alone.
Monitoring Load Tolerance
Appropriate load progression is indicated by:
• Symptom resolution within 24–48 hours
• Improved movement quality
• Progressive functional improvement
Signs of overload include:
• Persistent pain or swelling
• Movement compensations
• Decline in performance
Load must always respect tissue healing timelines and individual variability.
Pillar II: Dosage Progression
Defining Dosage
Dosage refers to the total therapeutic exposure to exercise, encompassing:
• Frequency (sessions per day/week)
• Intensity (effort level)
• Volume (sets, repetitions, duration)
• Rest intervals
Dosage determines the accumulated physiological stress, often more decisively than load alone.
Importance of Dosage Control in Rehabilitation
Two patients performing identical exercises with identical load may experience vastly different outcomes due to differences in dosage. Poor dosage control commonly leads to:
• Overuse symptoms
• Fatigue-related technique breakdown
• Reduced adherence
• Delayed recovery
Evidence-Based Dosage Parameters by Rehabilitation Goal
Strength Development
• Moderate to high intensity
• Lower repetitions
• Adequate rest between sessions
Endurance and Conditioning
• Lower intensity
• Higher repetitions or duration
• Shorter rest intervals
Motor Control and Early Rehabilitation
• Low intensity
• Very high repetition
• Frequent practice emphasizing quality
Cardiopulmonary Rehabilitation
• Dosage guided by physiological markers
• Duration progressed before intensity
Table 2. Dosage Characteristics by Therapeutic Objective
| Therapeutic Goal | Intensity | Volume | Frequency | Clinical Purpose |
| Strength | Moderate–high | Low–moderate | 2–3×/week | Increase force capacity |
| Endurance | Low–moderate | High | 3–5×/week | Improve fatigue resistance |
| Motor relearning | Low | Very high | Daily or multiple/day | Enhance neural adaptation |
| Conditioning | Individualized | Progressive | Regular | Improve aerobic capacity |
This table translates abstract exercise science concepts into clinically actionable dosage templates, aiding safe and goal-specific prescription.
Dosage Progression Strategies
• Increase repetitions before resistance
• Increase frequency before intensity in deconditioned patients
• Reduce rest intervals to increase work density
• Autoregulate using perceived exertion and symptom response
Dosage progression must remain flexible, accounting for daily variability in pain, fatigue, and recovery.
Pillar III: Specificity of Exercise Progression
The Principle of Specificity
The principle of specificity states that adaptations are specific to the nature of the training stimulus. In rehabilitation, this principle determines whether strength and capacity gains actually translate into meaningful functional improvement.
Dimensions of Specificity in Physiotherapy
• Movement specificity – joint angles and muscle sequencing
• Velocity specificity – slow vs fast movements
• Postural specificity – supine vs upright tasks
• Contextual specificity – stable vs variable environments
• Cognitive specificity – single-task vs dual-task demands
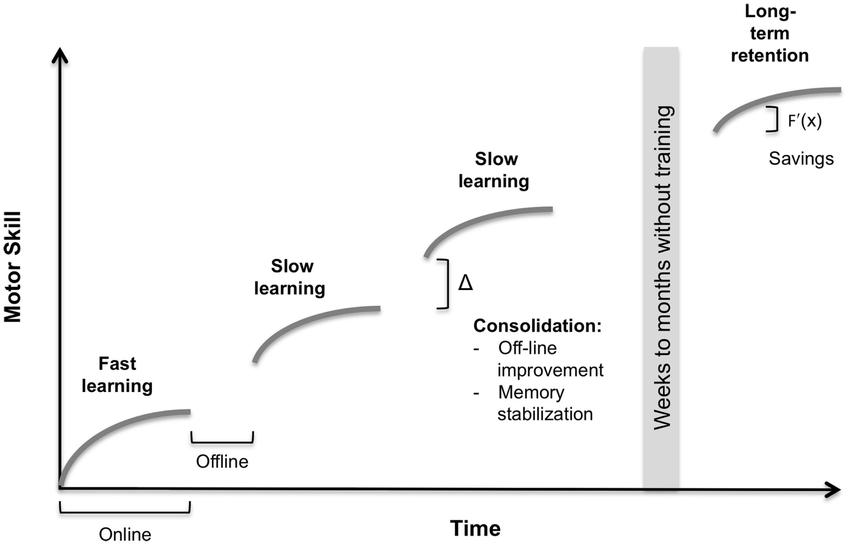
This visual demonstrates how task-specific training bridges the gap between impairment-level gains and participation-level function.
Progressing Specificity in Clinical Practice
Specificity should be progressed systematically:
• Isolated → integrated tasks
• Simple → complex movements
• Predictable → variable environments
• Assisted → independent performance
Specificity should only be increased once adequate load tolerance and dosage capacity are established, to avoid premature overload.
Integrating Load, Dosage, and Specificity: Clinical Reasoning in Action
Progression is not linear. Adjusting one variable often necessitates modification of others:
• Increasing specificity may require reducing load
• Increasing load may require reducing volume
• Increasing dosage may require simplifying task complexity
This flow-based visual supports clinical decision-making by showing how progression variables must be balanced rather than escalated simultaneously.
Application Across Rehabilitation Domains
Musculoskeletal Rehabilitation
Emphasis on graded loading, tissue tolerance, and functional transfer.
Neurological Rehabilitation
High repetition, task-specific practice with fatigue monitoring.
Cardiopulmonary Rehabilitation
Dosage-driven progression with physiological monitoring.
Geriatric Rehabilitation
Functional relevance, safety, and conservative progression.
Common Clinical Errors in Exercise Progression
• Advancing resistance without movement quality
• Increasing volume despite inadequate recovery
• Neglecting task specificity
• Applying generic protocols without individualization
Avoiding these errors requires continuous reassessment and outcome monitoring.
Evidence-based progression of therapeutic exercise is a core professional competency in physiotherapy. Mastery of load, dosage, and specificity allows clinicians to:
• Optimize tissue adaptation
• Enhance functional recovery
• Reduce adverse responses
• Deliver patient-centered, outcome-driven care
Progression is not about doing more—it is about doing what is appropriate, when it is appropriate, and for a clearly defined purpose.
References
- American College of Sports Medicine. (2021). ACSM’s guidelines for exercise testing and prescription (11th ed.).
- Shumway-Cook, A., & Woollacott, M. (2017). Motor control: Translating research into clinical practice.
- World Physiotherapy. (2023). Description of physical therapy practice.
- McArdle, W. D., Katch, F. I., & Katch, V. L. (2015). Exercise physiology.
- Cochrane Rehabilitation. (2022). Exercise therapy in rehabilitation.
- NICE. (2020). Rehabilitation after critical illness.