Introduction
Clinical reasoning is the central intellectual process that distinguishes professional physiotherapy practice from the mechanical application of techniques. It represents the structured yet flexible thinking process through which physiotherapists collect, interpret, and synthesize patient information to make justified clinical decisions. These decisions span the entire continuum of care, from initial assessment and diagnosis to intervention planning, progression, discharge, and long-term follow-up.
In modern healthcare systems characterized by increasing patient complexity, multimorbidity, resource constraints, and heightened accountability, robust clinical reasoning is not optional. It is fundamental to patient safety, therapeutic effectiveness, ethical practice, and professional autonomy. Errors in clinical reasoning are a major contributor to misdiagnosis, ineffective treatment, prolonged disability, and adverse events. Conversely, advanced reasoning skills are consistently associated with better outcomes, efficient care delivery, and enhanced patient satisfaction.
This revised article presents a comprehensive, text-based and copyright-safe exposition of clinical reasoning in physiotherapy practice. It integrates theoretical models, cognitive science principles, evidence-based practice, and real-world clinical application across specialties.
Defining Clinical Reasoning in Physiotherapy
Clinical reasoning in physiotherapy can be defined as the cognitive and metacognitive processes used by the clinician to integrate biomedical knowledge, movement science, clinical experience, patient values, contextual factors, and research evidence to make informed decisions about patient management.
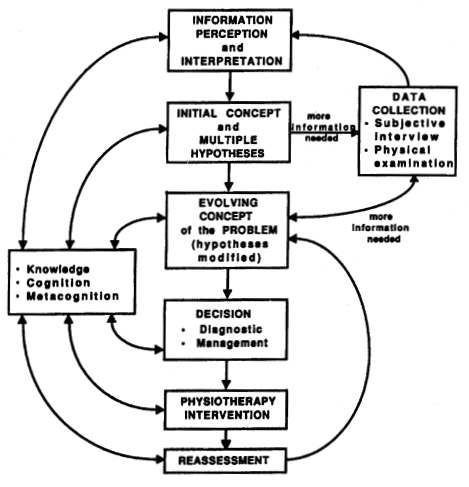
It is not a linear process. Rather, it is iterative, dynamic, and responsive to new information. Clinical reasoning involves:
-
Problem identification and prioritization
-
Hypothesis generation and testing
-
Decision-making under uncertainty
-
Reflection during and after action
-
Justification of clinical choices
Importantly, clinical reasoning is goal-directed. Every assessment question, physical test, and intervention choice should have a clear rationale linked to patient outcomes.
Theoretical Foundations of Clinical Reasoning



Clinical reasoning in physiotherapy is informed by multiple theoretical models. Expert clinicians do not adhere rigidly to one model; instead, they integrate several approaches depending on the clinical context.
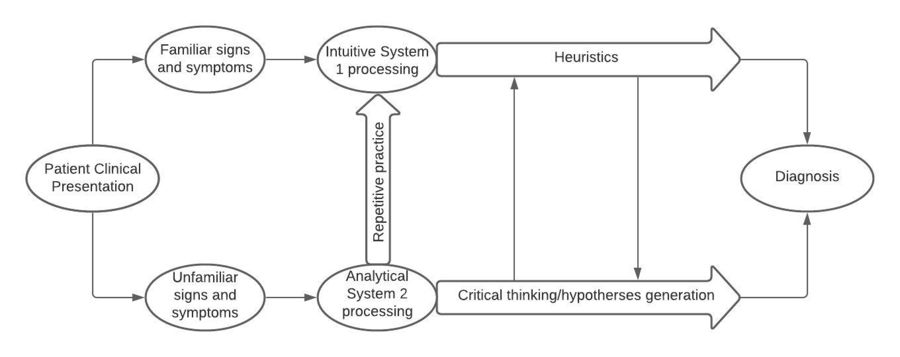
Hypothetico-deductive reasoning is a structured analytical approach in which the clinician generates multiple hypotheses early in the assessment and systematically tests them through targeted questioning and examination. This model is particularly important in complex, unfamiliar, or high-risk cases.
Pattern recognition relies on rapid identification of familiar clinical presentations based on prior experience. It enables efficient decision-making but carries a higher risk of cognitive bias if not balanced with analytical reasoning.
Narrative reasoning focuses on understanding the patient’s story, beliefs, expectations, psychosocial stressors, and lived experience of illness. This model is essential for patient-centered care, adherence, and management of chronic conditions.
Procedural reasoning guides the selection and sequencing of assessment tools and treatment techniques. While necessary, overreliance on procedural reasoning can reduce care to protocol-driven practice.
Ethical reasoning addresses moral and professional dilemmas, including informed consent, risk–benefit analysis, professional boundaries, and equitable resource allocation.
Pragmatic reasoning considers real-world constraints such as time, staffing, equipment, institutional policies, and socioeconomic factors.
Clinical Reasoning Across the Physiotherapy Process



Clinical reasoning is embedded throughout the entire physiotherapy care pathway.
Subjective assessment
Reasoning begins before the patient is physically examined. The clinician determines which information is essential, screens for red flags, assesses symptom behavior, and begins forming initial hypotheses. Effective questioning is selective and hypothesis-driven, not exhaustive.
Objective examination
Test selection is guided by prior hypotheses. Findings are interpreted for their reliability, validity, and clinical relevance. Inconsistencies prompt reassessment rather than forced conclusions.
Clinical diagnosis and problem formulation
Physiotherapists synthesize findings into a structured problem list that includes impairments, activity limitations, participation restrictions, and contextual factors, rather than focusing solely on tissue pathology.
Goal setting
Goals are reasoned collaboratively, balancing clinical feasibility with patient priorities. They must be specific, measurable, meaningful, and time-bound.
Intervention planning
Treatment choices are justified based on mechanism of action, evidence strength, patient capacity, risk profile, and expected dose–response relationship.
Reassessment and progression
Ongoing reasoning evaluates whether observed changes result from intervention, spontaneous recovery, or external factors, and whether modification or escalation of care is required.
Clinical Reasoning and Evidence-Based Practice

Evidence-based practice strengthens clinical reasoning but does not replace it. Research evidence provides population-level probabilities, not individualized certainty. Clinical reasoning determines how and whether evidence applies to the patient in front of the clinician.
Key reasoning considerations include:
-
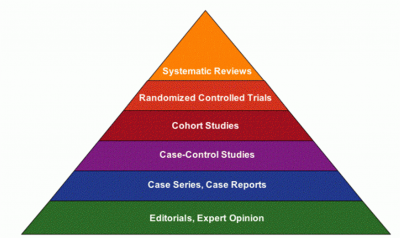
Quality and hierarchy of evidence
-
External validity and population relevance
-
Clinical significance versus statistical significance
-
Patient preferences, beliefs, and goals
-
Resource availability and feasibility
Strong clinical reasoning integrates evidence without becoming algorithmic or inflexible.
Cognitive Bias and Error in Clinical Reasoning

Clinical reasoning is inherently vulnerable to cognitive bias. Awareness of these biases is essential for safe practice.
Common biases include:
-
Anchoring bias
-
Confirmation bias
-
Availability bias
-
Premature closure
-
Overconfidence bias
Mitigation strategies include reflective practice, deliberate consideration of alternative hypotheses, peer discussion, structured reassessment, and use of validated outcome measures.
Clinical Reasoning in Complex and Specialized Contexts


In neurological rehabilitation, clinical reasoning emphasizes neuroplasticity, task specificity, motor learning principles, and recovery trajectories.
In critical care, reasoning prioritizes physiological stability, risk stratification, and interprofessional coordination.
In chronic pain management, reasoning integrates biopsychosocial frameworks, pain neuroscience education, and behavior change strategies.
In geriatrics, multimorbidity, frailty, cognition, and social context dominate decision-making.
Across all settings, linear reasoning is insufficient; adaptive and systems-based thinking is required.
Development of Clinical Reasoning Skills

Clinical reasoning develops progressively. Novices rely heavily on rules and protocols, while experts demonstrate fluid integration of pattern recognition and analytical reasoning, supported by reflection.
Effective development strategies include:
-
Case-based and problem-based learning
-
Simulation and deliberate practice
-
Mentorship and guided reflection
-
Structured clinical reasoning frameworks
Clinical reasoning is a lifelong competency that must evolve with evidence, technology, and patient expectations.
Documentation as an Expression of Clinical Reasoning
Clinical documentation should reflect reasoning, not merely actions. High-quality documentation articulates:
-
Rationale for assessment choices
-
Clinical interpretation of findings
-
Justification for interventions
-
Logic behind progression or discharge decisions
Clear documentation enhances continuity of care, legal defensibility, and professional credibility.
Future Directions
Digital health technologies, clinical decision support systems, and artificial intelligence will increasingly inform physiotherapy practice. However, they do not replace clinical reasoning. Human judgment, ethical discernment, and contextual understanding remain irreplaceable.
The future of physiotherapy depends not on technique proliferation, but on strengthening clinical reasoning capacity across all levels of practice.
Conclusion
Clinical reasoning is the intellectual foundation of physiotherapy practice. It transforms scientific knowledge and technical skill into individualized, ethical, and effective patient care. Mastery of clinical reasoning distinguishes expert clinicians, reduces error, enhances outcomes, and safeguards professional autonomy. Continuous refinement of this competency is essential for contemporary and future physiotherapy practice.
Key References
Higgs J, Jones M, Loftus S, Christensen N. Clinical Reasoning in the Health Professions. 4th ed. Elsevier; 2019.
Edwards I, Jones M, Carr J, Braunack-Mayer A, Jensen GM. Clinical reasoning strategies in physical therapy. Physical Therapy. 2004.
Jensen GM, Gwyer J, Hack LM, Shepard KF. Expertise in physical therapy practice. Physical Therapy. 2000.
Elstein AS, Schwartz A. Clinical problem solving and diagnostic decision making. BMJ. 2002.
World Health Organization. International Classification of Functioning, Disability and Health (ICF). 2001.